a Department of Cardiology, Bern University Hospital (Inselspital), University of Bern, Switzerland; b ARTORG Centre for Biomedical Engineering Research, University of Bern, Switzerland
The goal of this article is to provide an overview on contemporary pacing techniques, their most common uses and limitations.
Introduction
In the past decade, cardiac pacing techniques evolved significantly – resulting in a large variety of available approaches that are used to tailor stimulation individually to the patient’s needs. Subsequently, the European Society of Cardiology has recently updated guidelines on cardiac pacing [1]. The goal of this mini-review is to provide an overview on contemporary pacing techniques, their most common uses and limitations.
Conventional right ventricular pacing
Right ventricular (RV) apical pacing has been the cornerstone of cardiac pacing for bradycardia-induced symptoms since its introduction. It is an established and effective therapy restoring heart rate and improving bradycardia-induced symptoms. The longevity of current pacemaker (PM) systems is in many cases more than a decade.
Transvenous RV pacing is widely available in hospitals throughout Switzerland due to its ease of implantation. Venous access is gained via the left or right subclavian vein, the PM lead is advanced into the RV cavity and connected to a pulse generator in the pectoral pocket. Dual chamber systems, featuring an additional atrial lead, allow atrioventricular (AV) synchrony. Complications within two month after implantation requiring an intervention (e.g. significant pocket haematoma, lead dislocation or perforation, pneumothorax, acute infection) are under 5% in the hands of experienced operators [2]. The adoption of refined implantation techniques such as axillary vein (instead of subclavian vein) puncture or septal (instead of apical) lead placement is strongly recommended [3] and has the potential to further reduce adverse events such as pneumothoraces or cardiac perforations. Transvenous PM implantation is considered a relatively safe long-term therapy. However, more than 20% of patients experience complications within five years after implantation, mostly related to the pacing leads [2]. Besides system failures, patients may also develop pacing-induced cardiomyopathy due to unphysiological ventricular stimulation. Thus, recent innovations in the field aimed at removing the Achilles’ heel of conventional systems (leadless pacing) or providing a more physiological way of ventricular activation (cardiac resynchronisation therapy [CRT] or conduction system pacing [CSP], i.e. His bundle pacing [HBP] or left bundle branch area pacing [LBBAP]).
Leadless pacing
In 2012, the first-in-man implantation of a right ventricular leadless pacemaker was performed. After initial setbacks due to implantation- and device-related adverse events, leadless pacemaker technology was soon shown to be effective [4]. The projected system longevity reaches more than eight years in most patients.
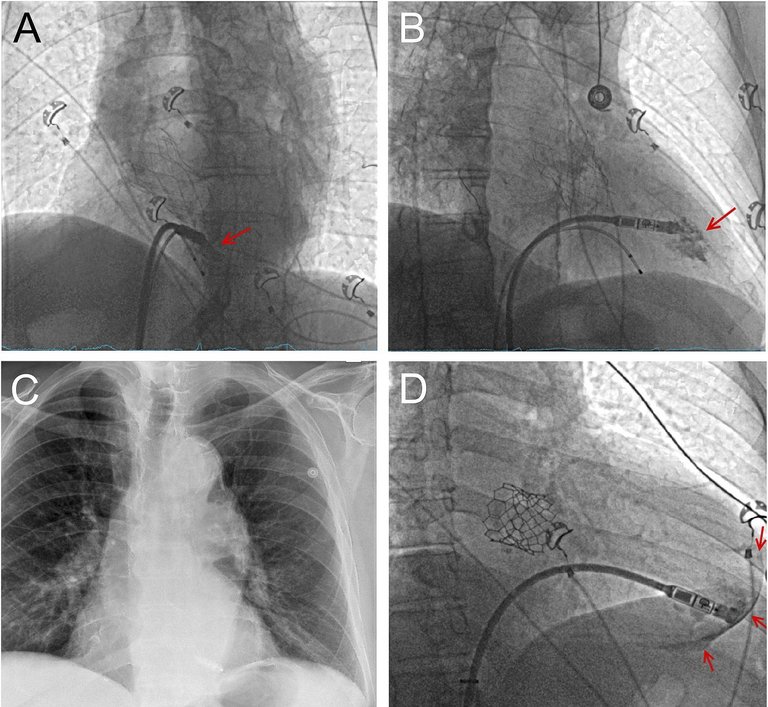
To implant a leadless pacemaker, access is gained via the femoral vein and the system is navigated to the interventricular septum, where it is anchored using a tine-based mechanism or a screw (fig. 1A-C). It can be programmed as a backup pacemaker or in VVIR (ventricular demand rate responsive) mode. During implantation of a leadless PM, caution is warranted, as cardiac perforations caused by the delivery catheter or the device may result in devastating complications requiring immediate cardiac surgery (fig. 1D). However, the overall complication rate of leadless PMs is presumably significantly lower compared to transvenous PMs [4] and appropriate training and sufficient experience results in excellent success rates and outcomes [5]. Naturally, lead-associated complications cannot occur and a subcutaneous pocket is not required, which almost eliminates device infections and the need for device removal. This is important, as percutaneous device extractions after a few years of implantation may be challenging due to encapsulation.
Figure 1: Panels A , B) Patient with intermittent complete AV block after transcatheter aortic valve implantation (TAVI) undergoing leadless pacemaker implantation. Temporary backup pacing is ensured via an electrophysiology catheter. Panel A shows a LAO view, panel B a RAO view. The red arrow shows the contrast medium, which illustrates that the PM is properly positioned at the interventricular septum. Panel C) Postoperative X-ray in p.a. projection after device release. Panel D) Different patient with increasing AV block I° (PQ >400 ms) after TAVI (RAO view). During device positioning, a crescent-shaped contrast medium deposit was seen (arrows), indicative for ventricular perforation. Pericardiocentesis, autotransfusion of circa 1.5 L blood and emergency sternotomy were performed and an RV rupture was sutured. After surgery, the patient recovered well and was dismissed from hospital five days after the complication with a transvenous pacemaker.
Recent innovations in leadless pacing technology have enabled these devices to provide a certain degree of atrio-ventricular synchrony in sinus rhythm. In one specific device, the atrial mechanical contraction can be sensed in the RV, allowing for atrial tracking up to a heart rate of 115 bpm. This may be sufficient for elderly patients with preserved left ventricular (LV) function and (intermittent) bradycardia due to AV block or impaired AV conduction. However, good atrial sensing can be difficult to achieve and suffers from limited efficacy at higher sinus rates [6]. Alternatively, the implantation of atrial and ventricular leadless PMs, which communicate wirelessly, have been proposed to perform true dual-chamber pacing [7]. Such systems currently undergo first-in-man trials and offer better AV synchrony, albeit not as good as conventional systems.
Leadless pacing should be considered for patients at increased risk for device infections (e.g. patients on haemodialysis) or patients without upper extremity venous access [1]. Patients presenting with an AV block after transcatheter aortic valve implantation may also be suitable candidates taking life expectancy into account. On the other hand, patients with impaired left ventricular function should generally not be implanted with a leadless PM. While leadless CRT in such patients has been proven feasible using an ultrasound-based transceiver, this remains a niche market due to significant failure rates and complications [8].
Cardiac resynchronization therapy (CRT) pacing
The MOST [9] and DAVID [10] trial reported harmful effects of chronic RV pacing attributable to ventricular dyssynchrony leading to a reduction of LV function, heart failure symptoms and a higher proportion of atrial fibrillation. This led to the programming of longer AV delays and development of algorithms aiming at RV pacing minimisation. On the other hand, long AV delays are not physiological and may result in diastolic mitral and tricuspid valve regurgitation. Therefore, more physiological ways of pacing are desired as this may be beneficial for a large proportion of patients.
Cardiac resynchronization therapy (CRT) is a well-established therapy with many large randomised clinical trials documenting its effectiveness in heart failure patients with severely reduced LV ejection fraction (LVEF) and broad QRS morphology, especially left bundle branch block (LBBB) [11, 12]. Moreover, in the BLOCK HF trial [13], patients with AV block and a LVEF of 35%-50% demonstrated a reduction in the composite endpoint of mortality, heart failure hospitalisation and echocardiographic worsening of heart failure compared to patients receiving a conventional PM.
Venous access for CRT is gained in the same way as during conventional PM implantation. In contrast to conventional PMs, an additional coronary sinus lead is inserted to be able to pace the posterolateral wall of the LV. To be able to place the lead, the coronary sinus is cannulated and in an over-the-wire technique, a quadripolar pacing lead is advanced into a suitable target vein. All leads are connected to a generator in the subcutaneous pocket. Due to the additional lead and implantation time, acute complications (e.g. pneumothorax, pocket haematoma, phrenic nerve stimulation, lead dislocation, cardiac perforation, infection) and adverse events during follow-up are more frequent compared to conventional PMs [14]. Moreover, the additional lead causes increased battery drain, which is often aggravated by disproportionally elevated LV pacing thresholds. Thus, battery longevity of CRT devices is generally lower compared to conventional PMs and significant differences amongst device manufacturers are known.
A successful CRT implantation relies on a suitable anatomy of the coronary sinus branches to place the LV lead in a basolateral position. Concomitant phrenic nerve stimulation is a challenge that can often be overcome by choosing a different pacing pole configuration. Diseased myocardium or a scar at the target location may increase LV pacing thresholds to an inacceptable level or can result in slow conduction, leading to significant latency from the electrical stimulus to the ensuing myocardial contraction. This needs to be addressed by adjusting the device programming. Finally, despite improvements of the implant technique, invention of quadripolar LV leads and sophisticated device algorithms optimising the AV and VV intervals automatically, more than one third of the patients do not respond to CRT. Together with less established potential CRT indications such as patients with QRS duration under 150 ms and/or PR prolongation in patients with reduced LVEF, this motivates a demand for an even more physiological pacing modality such as conduction system pacing.
Epicardial pacing
Young patients suffering from congenital heart disease or patients undergoing surgery due to endocarditis or tricuspid valve disease may benefit from an epicardial pacing lead in conjunction with cardiac surgery [1]. While surgical lead implantation in these patients is a valuable option, the relevance of surgical lead implantation as a bailout strategy after failed CRT implantation is decreasing [1]. Epicardial devices are not magnetic resonance imaging dependent, which – to date – remains a limitation. Although the availability of a suitable target vein can sometimes prevent successful CRT implantation, alternative minimally-invasive options are desired and, again, conduction system pacing provides a way out.
Conduction system pacing (CSP)
The basic idea of conduction system pacing – encompassing His bundle (HBP) and left bundle branch area pacing (LBBAP) – is to use the heart’s intrinsic conduction system to stimulate the myocardium in the most physiological way possible. Even in patients with complete AV block or bundle branch blocks, the conduction system at the level of the His bundle and infra-hisian may still be largely intact. CSP was already performed for the first time more than 20 years ago. The general implantation approach is similar to conventional PMs, but placing a lead in the conduction system is more challenging. The introduction of three-dimensional guiding sheaths (allowing to reach the target area better) has increased the interest in CSP in the past few years. Nonetheless, an electrophysiology lab with 12-lead ECG and advanced mapping/pacing capabilities and specifically trained implanters are required for CSP. The challenges do not end after the implantation since the conduction system lead can be connected to the right atrial, RV or LV port of the PM. Depending on the setting and the specific needs of the patient, this increases the complexity of device programming. Moreover, device follow-ups are more time-consuming and require a 12-lead ECG for threshold testing as the conduction system lead may pace multiple structures (e.g. conduction system and working myocardium) simultaneously, each exhibiting a separate pacing threshold. A proper identification of these individual thresholds is crucial for the tailored programming of CSP systems [15]. In the following paragraphs, we present the individual particularities of HBP and LBBAP pacemakers.
His bundle pacing (HBP)
During implantation of a His bundle pacing lead, venous access is preferably gained via the left side. A conventional RV lead may be considered either as a temporary backup lead during the implantation procedure (in case of temporary iatrogenic AV block) or as a definitive backup lead. The target area is mapped using designated three-dimensional fixed or steerable His sheaths. The conduction system includes the AV node, the His bundle and the right and left bundle. Predestined fibres for the right, left anterior and left posterior bundles covered by fibrous tissue penetrate from the AV node into the interventricular septum. The target area for HBP are those fibres in the atrial part and the penetrating bundle, which is about 2-8 mm long and 1 mm thick. Most commonly, a lumenless 4.1F lead with a 1.8 mm long fixed helix (SelectSecure™ 3830, Medtronic, United States) is advanced through the sheath allowing mapping of the target area in a unipolar fashion until a His bundle potential can be recorded. The lead is fixated by a few turns of the whole lead. An atrial lead is added, if the patient is in sinus rhythm. Whether a permanent RV backup lead is implanted, depends on the clinical situation, but it is recommended in patients undergoing a pace-and-ablate strategy [1].
The electrical recruitment of the conduction system results in differences of HBP compared to conventional RV pacing. Paced QRS duration is shorter, increasing LV function and decreasing ventricular dyssynchrony and mitral regurgitation. This translates into superior clinical outcomes of HBP versus RV pacing. Patients with HBP experience a lower rate of heart failure hospitalisations and even lower all-cause mortality in observational studies [16]. Data on HPB versus CRT pacing are scarce, but HBP may be associated with similar rates of echocardiographic improvement and even greater reduction of the QRS duration compared to CRT in an on-treated analysis of a prospectively randomized trial [17].
However, HBP suffers from important limitations. Acute HBP implant success is around 75-80% and correction of a pre-existing LBBB may be achieved in under 50% of patients. Pacing thresholds of a HBP lead often is considerably higher, resulting in increased battery drain and earlier generator changes compared to conventional systems [18]. Lead dislocations or electrical dysfunction due to sensing or threshold issues may require lead revision (7% for HBP vs. 3% for RV pacing five years after implantation) [18].
Left bundle branch area pacing (LBBAP)
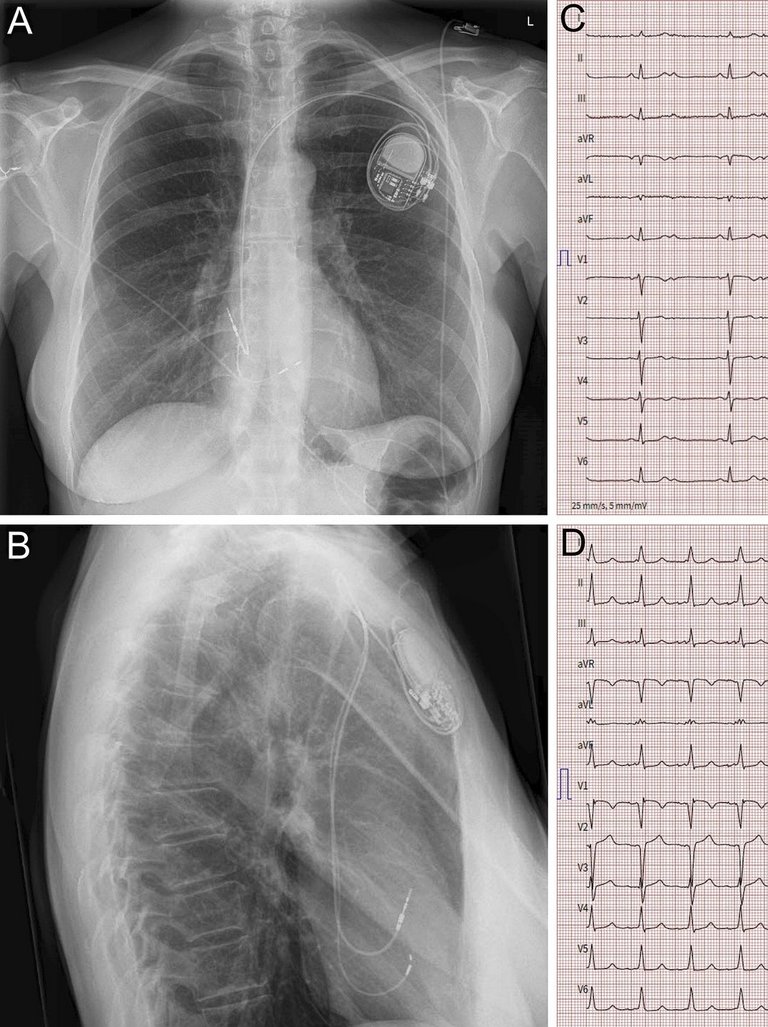
To implant the lead into the left bundle branch (LBB), the interventricular septum needs to be penetrated almost completely as the LBB lies in the LV subendocardium. To identify a suitable site for starting the lead drilling process on the right ventricular side, fluoroscopy and pace mapping are used. The lead is forced gradually through the septum using three-dimensional sheaths. Conventional stylet-driven or lumenless leads may be used. During drilling, continuous unipolar pacing is performed to monitor the fixation progress through the septum. Specific criteria on the 12-lead ECG indicative for LBB capture, repetitive unipolar impedance measurements and septography may provide information to avoid septal perforation. Positioning of the lead in the LBB usually results in relatively narrow QRS complexes (110-120ms, fig. 2), albeit the right bundle and the left anterior bundle may not always be captured in contrast to HBP, which – thus – may be considered the more physiological CSP variant. Combining the LBB lead with a conventional RV lead may further improve electrical activation of the ventricles.
Figure 2: Implantation of a conduction system pacemaker in a 62 year old patient without known heart disease and symptomatic 2:1 AV block. Panels A and B show the X-ray in p.a. (A) and lateral (B) projection. The ventricular lead is fixated in the interventricular septum in left bundle position. Panel C shows the ECG prior to implantation with 2:1 AV block and a narrow QRS complex. Panel D shows the ECG after implantation and bipolar ventricular simulation. The paced QRS duration of circa 110 ms and an r’ is visible in V1. The short R-wave peak time in V6 of circa 65 ms and a V6-V1 interpeak interval of circa 40 ms indicate successful recruitment of the conduction system.
Similar to HBP, LBBAP results in significant outcome differences in comparison to conventional RV pacing. Observational studies have demonstrated a lower rate of heart failure hospitalisations and lower all-cause mortality [19], attributed to a more physiologic ventricular activation (shorter QRS complexes). Importantly and in contrast to HBP, LBB leads exhibit similar or even superior electrical properties as conventional RV leads and only rarely dislocate [19]. Moreover, implant success rates seem to reach around 90% due to the larger target area.
Key points
Endovenous right ventricular (RV) septo-apical pacing has been the cornerstone for the treatment of bradycardia in patients with normal left ventricular (LV) function for many years.
Leadless pacemakers may provide atrioventricular synchrony and are particularly useful in older patients with preserved LV function or patients at increased risk for infections.
In case of cardiac resynchronisation therapy (CRT) implant failure or CRT non-response, conduction system pacing by His bundle or left bundle branch area pacing has become a valuable alternative.
Physiological pacing modalities may reduce heart failure, hospitalisations and mortality compared to RV pacing. Aiming at correction of an atrioventricular (AV) or bundle branch block with conduction system pacing seems reasonable.
Implant success rates and electrical pacing parameters are inferior in His bundle pacemakers compared to left bundle branch area (LBBAP) pacemakers. LBBAP systems may be easier to implant, but long-term clinical outcome data are lacking so far.
LOT-CRT and HOT-CRT
LBBAP optimized CRT (LOT-CRT) and HBP optimized CRT (HOT-CRT) systems are conventional CRT systems, which are complemented with an additional CSP lead (e.g. in the atrial port). This approach allows improvement of the ventricular activation time compared to LV pacing via a coronary sinus lead [20]. It may also be an option to further minimise QRS duration in selected patients suffering from relevant distal conduction disease. HOT-CRT and LOT-CRT implantations are feasible and safe but evidence is very limited so far.
Conduction system pacing in the European guidelines and in clinical practice
The recently updated guidelines on cardiac pacing [1] provide limited recommendations for CSP. HBP is mentioned as a bailout strategy after failed CRT implantation, an option in patients undergoing “pace-and-ablate” and as an alternative to RV pacing in patients with LVEF over 40% and over 20% anticipated ventricular pacing. The guidelines refrain from recommendations regarding LBBAP, LOT-CRT and HOT-CRT. However, very recent data indicate that LBBAP may also be valuable after failed CRT implantation [21] or could even provide superior clinical outcomes compared to CRT [22]. Although these are preliminary non-randomised data, which remain to be confirmed, a paradigm shift in cardiac pacing caused by CSP seems to be on the horizon.
Recommended references
1 Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J 2021;42:3427-3520.
3 Burri H, Starck C, Auricchio A, Biffi M, Burri M, D’Avila A, et al. EHRA expert consensus statement and practical guide on optimal implantation technique for conventional pacemakers and implantable cardioverter-defibrillators: endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), and the Latin-American Heart Rhythm Society (LAHRS). Europace 2021;23:983-1008.
5 Haeberlin A, Kozhuharov N, Knecht S, Tanner H, Schaer B, Noti F, et al. Leadless pacemaker implantation quality: importance of the operator’s experience. Europace 2020;22:939-946.
6 Neugebauer F, Noti F, van Gool S, Roten L, Baldinger SH, Seiler J, et al. Leadless atrioventricular synchronous pacing in an outpatient setting: Early lessons learned on factors affecting atrioventricular synchrony. Heart Rhythm 2022, online.
22 Vijayaraman P, Zalavadia D, Haseeb A, Dye C, Madan N, Skeete JR, et al. Clinical outcomes of conduction system pacing compared to biventricular pacing in patients requiring cardiac resynchronization therapy. Heart Rhythm 2022, online
Correspondence
Dr. med. Fabian Noti
Department of Cardiology Bern University Hospital
Freiburgstrasse 18
CH-3010 Bern
SWITZERLAND
References
1 Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J 2021;42:3427-3520.
2 Udo EO, Zuithoff NP, van Hemel NM, de Cock CC, Hendriks T, Doevendans PA, et al. Incidence and predictors of short- and long-term complications in pacemaker therapy: the FOLLOWPACE study. Heart Rhythm 2012;9:728-735.
3 Burri H, Starck C, Auricchio A, Biffi M, Burri M, D’Avila A, et al. EHRA expert consensus statement and practical guide on optimal implantation technique for conventional pacemakers and implantable cardioverter-defibrillators: endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), and the Latin-American Heart Rhythm Society (LAHRS). Europace 2021;23:983-1008.
4 Reynolds D, Duray GZ, Omar R, Soejima K, Neuzil P, Zhang S, et al. A Leadless Intracardiac Transcatheter Pacing System. The New England journal of medicine 2016;374:533-541.
5 Haeberlin A, Kozhuharov N, Knecht S, Tanner H, Schaer B, Noti F, et al. Leadless pacemaker implantation quality: importance of the operator’s experience. Europace 2020;22:939-946.
6 Neugebauer F, Noti F, van Gool S, Roten L, Baldinger SH, Seiler J, et al. Leadless atrioventricular synchronous pacing in an outpatient setting: Early lessons learned on factors affecting atrioventricular synchrony. Heart Rhythm 2022, online.
7 Bereuter L, Gysin M, Kueffer T, Kucera M, Niederhauser T, Fuhrer J, et al. Leadless Dual-Chamber Pacing: A Novel Communication Method for Wireless Pacemaker Synchronization. JACC Basic Transl Sci 2018;3:813-823.
8 Auricchio A, Delnoy PP, Butter C, Brachmann J, Van Erven L, Spitzer S, et al. Feasibility, safety, and short-term outcome of leadless ultrasound-based endocardial left ventricular resynchronization in heart failure patients: results of the wireless stimulation endocardially for CRT (WiSE-CRT) study. Europace 2014;16:681-688.
9 Sweeney MO, Hellkamp AS, Ellenbogen KA, Greenspon AJ, Freedman RA, Lee KL, et al. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation 2003;107:2932-2937.
10 Wilkoff BL, Cook JR, Epstein AE, Greene HL, Hallstrom AP, Hsia H, et al. Dual-chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: the Dual Chamber and VVI Implantable Defibrillator (DAVID) Trial. JAMA: the journal of the American Medical Association 2002;288:3115-3123.
11 Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. The New England journal of medicine 2004;350:2140-2150.
12 Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. The New England journal of medicine 2005;352:1539-1549.
13 Curtis AB, Worley SJ, Adamson PB, Chung ES, Niazi I, Sherfesee L, et al. Biventricular pacing for atrioventricular block and systolic dysfunction. The New England journal of medicine 2013;368:1585-1593.
14 Kirkfeldt RE, Johansen JB, Nohr EA, Jorgensen OD, Nielsen JC. Complications after cardiac implantable electronic device implantations: an analysis of a complete, nationwide cohort in Denmark. Eur Heart J 2014;35:1186-1194.
15 Bakelants E, Burri H. Troubleshooting Programming of Conduction System Pacing. Arrhythmia & electrophysiology review 2021;10:85-90.
16 Abdelrahman M, Subzposh FA, Beer D, Durr B, Naperkowski A, Sun H, et al. Clinical Outcomes of His Bundle Pacing Compared to Right Ventricular Pacing. J Am Coll Cardiol 2018;71:2319-2330.
17 Upadhyay GA, Vijayaraman P, Nayak HM, Verma N, Dandamudi G, Sharma PS, et al. On-treatment comparison between corrective His bundle pacing and biventricular pacing for cardiac resynchronization: A secondary analysis of the His-SYNC Pilot Trial. Heart Rhythm 2019;16:1797-1807.
18 Vijayaraman P, Naperkowski A, Subzposh FA, Abdelrahman M, Sharma PS, Oren JW, et al. Permanent His-bundle pacing: Long-term lead performance and clinical outcomes. Heart Rhythm 2018;15:696-702.
19 Sharma PS, Patel NR, Ravi V, Zalavadia DV, Dommaraju S, Garg V, et al. Clinical outcomes of left bundle branch area pacing compared to right ventricular pacing: Results from the Geisinger-Rush Conduction System Pacing Registry. Heart Rhythm 2022;19:3-11.
20 Jastrzębski M, Moskal P, Huybrechts W, Curila K, Sreekumar P, Rademakers LM, et al. Left bundle branch-optimized cardiac resynchronization therapy (LOT-CRT): Results from an international LBBAP collaborative study group. Heart Rhythm 2022;19:13-21.
21 Vijayaraman P, Herweg B, Verma A, Sharma PS, Batul SA, Ponnusamy SS, et al. Rescue left bundle branch area pacing in coronary venous lead failure or nonresponse to biventricular pacing: Results from International LBBAP Collaborative Study Group. Heart Rhythm 2022, online.
22 Vijayaraman P, Zalavadia D, Haseeb A, Dye C, Madan N, Skeete JR, et al. Clinical outcomes of conduction system pacing compared to biventricular pacing in patients requiring cardiac resynchronization therapy. Heart Rhythm 2022, online.