A survival kit for busy clinicians within the "SGLT2 inhibitors’ data jungle".
We read with interest the review article by Maeder, Rickli, and Buser on the role of sodium-glucose co-transporter 2 (SGLT2) inhibitors in heart failure [1]. During the last decade, nine large randomised trials testing the efficacy of three different compounds with respect to cardiovascular and renal endpoints have been published and others are expected soon (e.g. EMPA-Kidney trial investigating empagliflozin in patients with chronic kidney disease). Although the interest in SGLT2 inhibitors has paralleled the increasing evidence of beneficial effects, clinicians might also be confused by the rapidly growing body of evidence with (many) consistencies and (some) contradictory results. This "jungle" of results might discourage clinicians from selectively using SGLT2 inhibitors. Indeed, although we acknowledge that, at least to some degree, a "class effect" of SGLT2 inhibitors likely exists, relevant differences in study design, tested end-points and results preclude the generalisability of the observed findings to all compounds. Of note, the clinical setting (e.g., primary vs secondary cardiovascular prevention), the proportion of diabetic patients (ranging from 42% to 100%), the range of prevalence of arteriosclerotic cardiovascular disease (from 35% to 100%) and heart failure (from 10% to 100%) substantially differ across the trials.
Hence, cautious use of the tested compound in the appropriate setting seems the most reasonable approach. Accordingly, the 2021 European Society for Cardiology (ESC) guidelines for the treatment of heart failure recommend the use of dapagliflozin or empagliflozin for patients with reduced ejection fraction, since only for these two compounds dedicated trials in heart failure exist [2]. Similarly, in patients with preserved or mildly reduced ejection fraction, both compounds showed beneficial prognostic effects and they will likely be included in future guidelines updates.
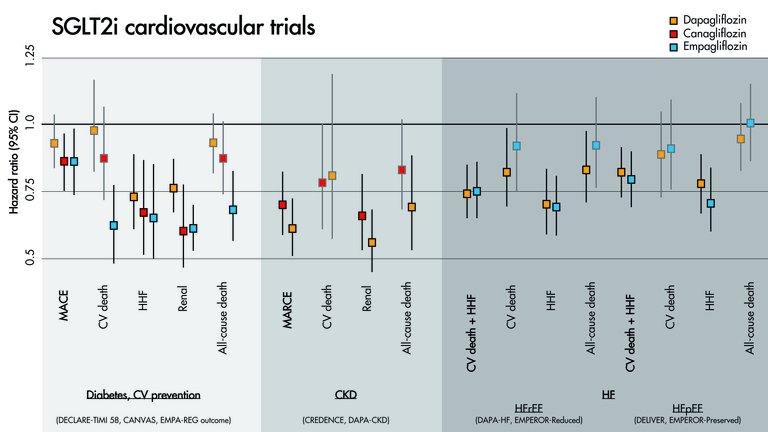
As survival kit for busy clinicians within the "SGLT2 inhibitors' data "jungle", we provide here the cornerstones of the largest published randomised clinical trials (table 1) and a figure visualising the results for the main cardiovascular and renal endpoints tested (fig. 1). With this primer, we hope to facilitate the optimal use of SGLT2 inhibitors in daily clinical care of cardiovascular patients.
Table:
Main characteristics of the large published randomised clinical trials investigating SGLT2 inhibitors for cardiovascular and renal endpoints.
Setting
Diabetes
Diabetes
Diabetes
Diabetes and CKD
CKD
HF
HF
HF
HF
Drug
Dapagliflozin
Canagliflozin
Empagliflozin
Canagliflozin
Dapagliflozin
Dapagliflozin
Empagliflozin
Dapagliflozin
Empagliflozin
Trial
DECLARE-TIMI-58
CANVAS
EMPA-REG outcome
CREDENCE
DAPA-CKD
DAPA-HF
EMPEROR-REDUCED
DELIVER
EMPEROR-PRESERVED
Year
2019
2017
2015
2019
2020
2019
2020
2022
2021
Cohort
Diabetes, ASCVD or multiple risk factors, eGFR ≥60 ml/min
Diabetes, ASCVD or multiple risk factors, eGFR ≥30 ml/min