The diagnostic accuracy of an ECG algorithm for predicting the infarct-related artery in acute inferior STEMI.
Introduction
Inferior ST-segment elevation myocardial infarction (STEMI) is due to an acute occlusion of the right coronary artery (RCA) in up to 80% of affected patients, whereas occlusion of the left circumflex coronary artery (LCX) is responsible for the remaining cases [1]. Immediate diagnosis and therapy of inferior STEMI is critical to achieve optimal patient outcomes [2].
Several years ago a simple ECG algorithm for predicting the infarct-related artery (IRA) in acute inferior STEMI was proposed [3]. The authors suggested that the presence of ST-segment elevation in lead III exceeding that in lead II when combined with ST-segment depression in leads I, aVL or both (RCA algorithm) represents a powerful predictor of occlusion of the RCA as culprit lesion of the acute inferior STEMI. In a review of data from four studies including their own, Zimetbaum et al. proposed sensitivity and specificity values of 90% and 71%, as well as positive and negative predictive values of 94% and 70% for this ECG algorithm [1, 3–6]. However, all of the studies included in the review of Zimetbaum et al. were relatively small trials of between 41 and 83 patients each [3–6]. Moreover, most of these studies were performed in the thrombolytic era; thus, only a minority of included patients underwent immediate coronary angiography and primary percutaneous coronary intervention (PPCI). Indeed, the excellent sensitivity values for the ECG algorithm reported by Zimetbaum et al. could not be reproduced in a larger cohort of Dutch patients with acute inferior STEMI who underwent PPCI [7].
Therefore, the present study was performed to further investigate the reliability of this ECG algorithm in daily clinical practice in a large cohort of patients with acute inferior STEMI undergoing PPCI.
Methods
The ECGs of all patients who presented with acute inferior STEMI (as indicated by typical symptoms consistent with myocardial ischaemia including persistent chest pain and ST-segment elevation of >1 mm in at least two contiguous inferior leads) to the Kantonsspital Graubuenden in Chur, Switzerland and underwent emergency coronary angiography / PPCI from January 2006 to December 2013 were analysed retrospectively. Preprocedural 12-lead ECGs, based on which diagnosis of acute inferior STEMI and decision for immediate transfer to the cardiac catheterisation laboratory were made, were analysed by two independent cardiologists unaware of the angiographic findings. According to previous publications, ST-segment elevation in lead III exceeding lead II was defined as a ratio of elevation in lead III:II of >1 and ST-segment depression in leads I and/or aVL was defined as >1 mm of depression under baseline [1, 3]. Patients with a missing ECG prior to the procedure as well as patients presenting with a subacute inferior STEMI (indicated by the patient`s history and the presence of negative T-waves in the inferior leads) were excluded from the analysis. In a second step, the results of the ECG analysis were compared with the angiographic findings. Twenty-eight-day all cause mortality data were collected by chart review or by telephone inquiry of the patients or their general practitioners.
Mean values ± standard deviation and proportions of the patient characteristics were calculated. Sensitivity and specificity, as well as positive and negative predictive values, were calculated by using standard methods. For comparison of nominal data we used a chi-square test. Statistical analyses were done by using IBM® SPSS Statistics®, Version 22. A p-value of <0.05 was considered statistically significant.
Results
A total of 356 patients (mean age 61.7 ± 10.2 years) with acute inferior STEMI were included in the present study. Of these, 273 (76.7%) were men. The RCA was the infarct-related artery in 272 (76.4%) patients and the LCX in 76 (21.4%) patients. In 4 (1.1%) patients inferior STEMI was caused by distal occlusion of a large left anterior descending coronary artery (LAD) and in 4 (1.1%) patients a Ramus intermedius was the culprit artery.
Of the 272 patients with the RCA as infarct-related artery, 212 had a true positive ECG algorithm in the index ECG, corresponding to a sensitivity of 78% (95% confidence interval [CI] 72–82%), whereas of the 84 patients with another infarct-related artery only 42 had a true negative ECG algorithm, corresponding to a specificity of 49% (95% CI 38–61%) (fig. 1, table 1). Positive and negative predictive values of the ECG algorithm were 83% (95% CI 78–87%) and 41% (95% CI 31–51%), respectively (table 1).
Table 1
Comparison of the diagnostic accuracy of the proposed ECG algorithm between different publications.
Authors
Sensitivity
Specificity
PPV
NPV
Zimetbaum PJ, et al. [1]
90%
71%
94%
70%
Verouden NJ, et al. [7]
70%
72%
90%
39%
Buchmann B, et al.
78%
49%
83%
41%
PPV = positive predictive value; NPV = negative predictive value
Overall, 10 (2,8%) patients died within the first 28 days after admission to our hospital for acute inferior STEMI. Twenty-eight-day mortality was similar in men and women (n = 8, 2,9% vs n = 2, 2.4%, p = 0.933). Also, no significant difference was found in 28-day mortality among patients with the RCA (n = 7; 2,6%) or another coronary artery (n=3; 3,6%) as the infarct-related artery (p = 0.629). Of the 254 patients with a positive ECG-algorithm, 9 (3.5%) patients died during the observation period, whereas of those with a negative ECG algorithm only 1 (1.0%) patient died within 28 days after hospital admission (p = 0.186).
Discussion
Coronary angiography represents the gold standard for determining the infarct-related artery in patients with acute STEMI. However, the ECG remains a crucial tool in the diagnosis of patients with acute STEMI [2]. In the present study we could not reproduce the excellent diagnostic accuracy of an ECG algorithm for predicting the infarct-related artery in patients presenting with acute inferior STEMI reported by others [1, 3]. The sensitivities and specificities found in our study were significantly lower than those observed in the smaller populations in which they were developed. The sensitivity value found in our population was more or less in line with that found by Verouden et al. in a similar study published 10 years ago [7]. However, in contrast to the findings of Verouden and coworkers, specificity of the proposed ECG algorithm was markedly lower in our cohort (see table 1). Based on our results, the positive predictive value of a positive ECG-algorithm is lower than those proposed be both, Zimetbaum et al. and Verouden et al., whereas the negative predictive value of our Swiss cohort was similar to the one found in the Dutch population (table 1).
Previous data indicate that patients with myocardial infarctions in the LCX territory have worse outcomes than patients with RCA-related myocardial infarctions [8]. At least with regard to 28-day mortality, we could not confirm this finding. Notably, we observed a certain trend towards a higher 28-day mortality in patients with a positive ECG algorithm, irrespective of the affected culprit artery. Thus, it can be speculated that a positive ECG algorithm may serve as a marker of the amount of myocardium at risk. However, we are aware of the fact that our study cohort was still relatively small and, therefore, our 28-day mortality results should be interpreted with caution.
Our study suffers from the known limitations of a retrospective study. Thus, unfortunately, we were not able to report reliable information with regard to baseline characteristics, such as risk factors, history of prior coronary events and medication of the included patients at the time of the index event. Also, in the present study we did not differentiate between the dominance type of coronary supply in patients with acute inferior STEMI. Therefore, our data do not allow ta statement as to whether the performance of the proposed ECG algorithm could be influenced by the type of coronary supply dominance. Acute occlusion of a dominant RCA is usually associated with larger areas of myocardium at risk than occlusion of a non-dominant RCA. On the other hand, the same holds true for patients with a dominant LCX. Thus, it may be speculated that sensitivity and specificity values of the proposed ECG algorithm could be affected by the type of coronary supply dominance. Notably, however, in the study by Verouden et al., sensitivity values of the ECG algorithm were not altered when analysis was restricted to patients with a dominant RCA [7].
More than a decade ago early and accurate identification of the infarct-related artery on the ECG was considered crucial for guiding decisions regarding treatment, including the urgency of coronary revascularisation, in patients with STEMI [1]. However, since then the therapeutic strategy in patients with STEMI has changed and, to date, immediate coronary reperfusion, either by thrombolysis or ideally – if promptly available – by PPCI, represents the mainstay of therapy in all patients with acute STEMI irrespective of STEMI localisation or the presumed infarct-related artery [2]. Notably, prehospital treatment of STEMI patients has also changed within the last decades. For example, routine use of nitrates and beta-blockers is not recommended in current guidelines anymore [2]. Therefore, nowadays the correct electrocardiographic identification of the in patients with inferior STEMI has become of less importance and should not guide or even delay reperfusion measures.
In summary, given its suboptimal diagnostic reliability and the lack of therapeutic consequences in patients with acute inferior STEMI and a clear indication for urgent reperfusion therapy, the clinical relevance of the proposed criteria is questionable. Thus, based on our findings we cannot recommend the use of this ECG algorithm in todays clinical practice.
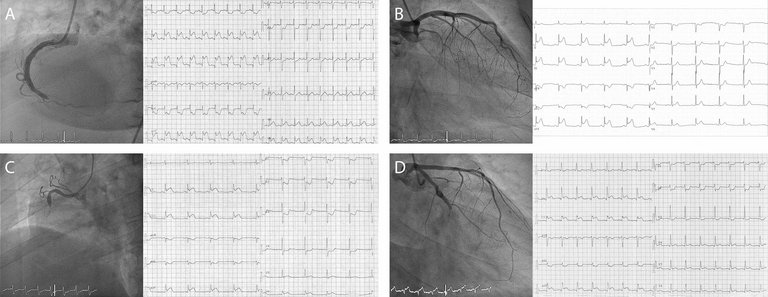
Figure 1
Examples of coronary angiograms and corresponding ECGs in patients with acute inferior ST-segment elevation myocardial infarction (STEMI). A positive ECG algorithm is defined as a ratio of ST-segment elevation in lead III:II of >1 and ST-segment depression in leads I and/or aVL >1 mm under baseline.
A. Acute inferior STEMI due to occlusion of the distal right coronary artery (RCA) with a true-positive ECG algorithm.
B. Acute inferior STEMI due to occlusion of the proximal left circumflex coronary artery (LCX) with a true-negative ECG algorithm.
C. Acute inferior STEMI due to occlusion of the mid RCA with a false-negative ECG algorithm.
D. Acute inferior STEMI due to occlusion of the mid LCX with a false-positive ECG algorithm.
Disclosure statement
No financial support and no other potential conflict of interest relevant to this article was reported.
2. The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77. http://dx.doi.org/10.1093/eurheartj/ehx393PubMed 0195-668X
3. . Usefulness of ST-segment elevation in lead III exceeding that of lead II for identifying the location of the totally occluded coronary artery in inferior wall myocardial infarction. Am J Cardiol. 1998 Apr;81(7):918–9. http://dx.doi.org/10.1016/S0002-9149(98)00013-7PubMed 0002-9149
4. . Electrocardiographic differentiation of occlusion of the left circumflex versus the right coronary artery as a cause of inferior acute myocardial infarction. Am J Cardiol. 1987 Sep;60(7):456–9. http://dx.doi.org/10.1016/0002-9149(87)90285-2PubMed 0002-9149
5. . ST segment depression in lateral limb leads in inferior wall acute myocardial infarction. Implications regarding the culprit artery and the site of obstruction. Eur Heart J. 1995 Nov;16(11):1549–53. http://dx.doi.org/10.1093/oxfordjournals.eurheartj.a060776PubMed 0195-668X
6. . New electrocardiographic criteria for predicting either the right or left circumflex artery as the culprit coronary artery in inferior wall acute myocardial infarction. Am J Cardiol. 1997 Nov;80(10):1343–5. http://dx.doi.org/10.1016/S0002-9149(97)00678-4PubMed 0002-9149
7. Distinguishing the right coronary artery from the left circumflex coronary artery as the infarct-related artery in patients undergoing primary percutaneous coronary intervention for acute inferior myocardial infarction. Europace. 2009 Nov;11(11):1517–21. http://dx.doi.org/10.1093/europace/eup234PubMed 1532-2092
8. Circumflex artery-related acute myocardial infarction: limited ECG abnormalities but poor outcome. Neth Heart J. 2007;15(9):286–90. http://dx.doi.org/10.1007/BF03086001PubMed 1568-5888