His refractory atrial extrastimulus can help for differential diagnosis between atrioventricular nodal reentrant tachycardia and junctional tachycardia.
Case presentation
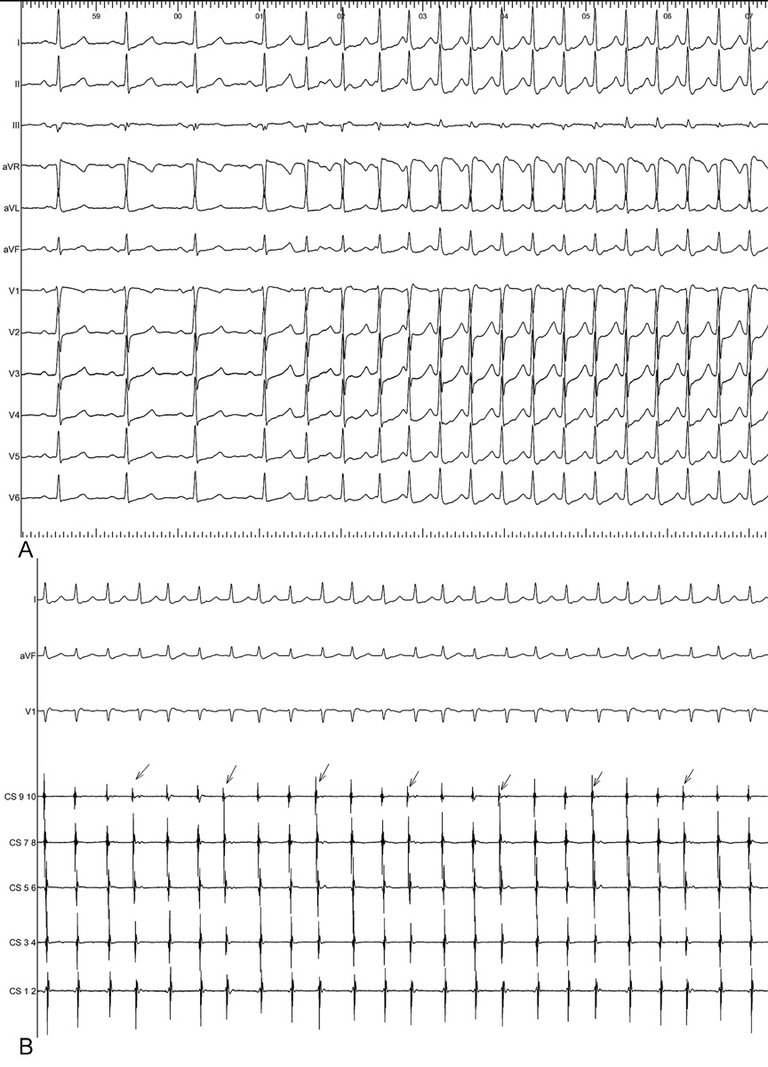
An 80‐year‐old woman with a 4-month history of frequent palpitations was admitted to our centre. The palpitations had an abrupt onset and termination. A 72-hour ECG recorded eight episodes of narrow complex supraventricular tachycardia, with slightly varying RR intervals. Since beta-blockers and verapamil could not control the tachycardia, we performed an electrophysiological study. In the electrophysiology laboratory, the patient showed a spontaneous, narrow QRS complex tachycardia resembling the clinical tachycardia (fig. 1A). Frequent premature atrial complexes (PACs) during the tachycardia were identified after placement of the coronary sinus catheter, resulting in a varying RR interval, as shown in figure 1B (arrows indicate the PACs).
Figure 1
A. The 12-lead ECG showed a narrow QRS complex tachycardia spontaneously starting before catheter introduction. B. The CS catheter recorded frequent PACs during tachycardia, resulting in slightly varying RR intervals (paper speed 25 mm/s). CS = coronary sinus (1-2 = distal, 9-10 = proximal).
After introduction of right ventricular apex and His catheters, the endocardial signals during tachycardia were as shown in figure 2. A short ventriculo-atrial interval (5 ms) excluded orthodromic atrioventricular reentrant tachycardia (AVRT). Before any electrophysiological manoeuvres, we observed PACs during the tachycardia. The His-His (H-H) interval was unchanged in the first QRS complex after the PAC. The next His was advanced 20 ms by the PACs, which excluded junctional tachycardia because PACs did not affect the His refractory period during junctional tachycardia. The spontaneous PACs occurred during the His refractory period, which could be identified in the His proximal electrode. As a result, the PACs were conducted anterogradely via a slow pathway during atrioventricular nodal reentrant tachycardia (AVNRT). The comparatively slow subsequent His perturbation (H-H 340 ms), in contrast to the short atrial-atrial (A-A) interval in the coronary sinus (A-A 310 ms), was interpreted as involvement of decremental slow pathway conduction.
Figure 2
Endocardiogram of tachycardia with timely PAC. The timely PAC during His refractoriness advanced the next His by 20 ms and reset the tachycardia due to the anterograde slow pathway conduction. Local atrial activation is indicated by a blue arrow on the proximal His electrode. Advancement of the next His by the His-refractory PAC indicated typical AVNRT and excluded junctional tachycardia.
Ventricular entrainment was performed during tachycardia, and a V-A-V response with PPI-TCL (post pacing interval – tachycardia cycle length) of 134 ms was achieved (fig. 3) [1, 2]. When the tachycardia was terminated by overdrive pacing, programmed stimulation was performed before ablation. The baseline electrophysiological parameters and characteristics are shown in table 1. Figure 4 shows that the AVNRT was induced by atrio-Hisian (AH) jump and following echo beat. AVNRT was diagnosed, with the exclusion of other supraventricular tachycardias, including atrial tachycardia and orthodromic AVRT. As a result, slow pathway ablation was carried out, and sustained slow junctional rhythm was obtained during ablation. No tachycardia was induced after that.
Figure 3
Ventricular entrainment manoeuvre during tachycardia to identify a V-A-V response. Ventricular overdrive pacing from the right ventricle (RV) with a cycle length of 340ms confirmed the entrainment. The last entrained atrial depolarisation (A) registered by the CS catheter was conducted to the ventricle via the slow pathway, resulting in a V-A-V response. Note the post pacing interval-TCL was >115ms.
Figure 4
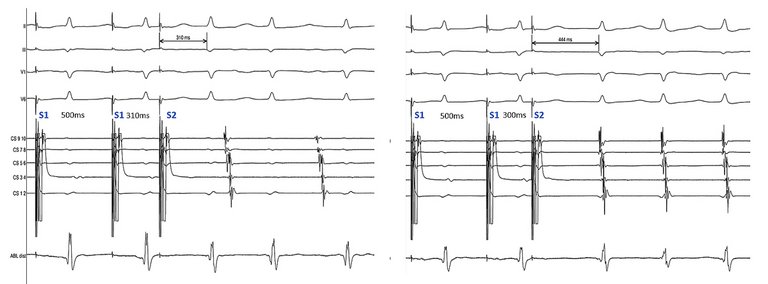
Programmed atrial extrastimulus pacing manoeuvre during sinus rhythm to identify an AH jump and echo beat followed by typical AVNRT. AVNRT was induced by a jump (134 ms) and echo beat at A1A2 (S1S2) coupling interval range of 310 ms to 300 ms, indicating a typical AVNRT. Since the programmed atrial extrastimulus testing was performed after the His catheter was replaced by the ablation catheter, the AH jump was derived from the difference between the two AV intervals.
Table 1
Baseline electrophysiological parameters and pacing manoeuvres. AV nodal effective refractory period (AVNERP) was measured at progressively shortening extrasystole intervals of 10 ms following eight drive trains at 500 ms. All measurements were made under baseline conditions without administration of isoprenaline. The lack of progressive fusion with decremental atrial pacing excluded ventricular preexcitation. VA decremental and concentric conduction (CS conduction sequence from proximal to distal) excluded a retrograde accessory pathway. VAV response to ventricular entrainment during tachycardia was used to exclude an atrial tachycardia.
His-refractory atrial extrastimulus can help differentiate between AVNRT and junctional tachycardia. Advancement, delay or termination of the subsequent beat by His-refractory atrial pacing indicates typical AVNRT [3]. His-refractory atrial pacing cannot affect a junctional tachycardia because of the refractoriness of His during the tachycardia. In the present patient, spontaneous PACs occurred at junctional depolarisation, i.e., His refractoriness. This timely His refractory PAC was manifested by the local atrial deflection after His signal on the proximal His electrogram. Furthermore, the PACs did not influence the immediate subsequent beat and did not change the corresponding H-H interval, as shown in figure 2. These observations demonstrated the electrophysiological mechanisms of AVNRT, with the exclusion of junctional tachycardia. Note that the patient had more frequent PACs during supraventricular tachycardia than during sinus rhythm. PACs during AVNRT were hidden in the T wave. Since the frequent PACs during tachycardia varied the RR intervals on the surface ECG, they might be misleading about the tachycardia mechanism [3]. At the same time, defined PAC morphology followed by AVNRT showed an inferior P wave axis and positive P wave in V1, aVL and the precordial leads, indicating high left atrium or right pulmonary vein origin. In this case, the fast ventricular rhythm might influence atrial vulnerability by increasing left atrial filling pressures due to atrioventricular synchronous contraction during AVNRT [4]. Other factors such as systemic volume or neurohormonal changes could not be excluded as predisposing factors for PAC inducibility.
In this patient, the resetting of the tachycardia following His-refractory PAC suggested slow pathway engagement (fig. 5) and AVNRT as the tachycardia mechanism. As shown in figure 2, the next His was advanced by the timely PAC with ventriculo-atrial linking.
Figure 5
Responses to His refractory PAC in the present case, a schematic view. Responses to His refractory PAC during AVNRT. Black lines showed the conduction through AVN, His (H), and atrium (A). Red lines showed PAC: it perturbed the next His via the slow pathway, resulting in AVNRT resetting.
From an educational perspective, two diagnoses have to be considered. Firstly, junctional tachycardia can also be perturbed by a PAC with immediate His advancement, but this PAC cannot reset the tachycardia itself. It is known that junctional tachycardia is a focal activity, rather than reentry. If the PAC occurs when His is refractory, the junctional tachycardia will not be affected. As a result, PAC timing is very important for distinguishing between a junctional tachycardia and AVNRT. Another differential diagnosis is a dual atrioventricular node response, which means two QRS complexes occur after a single PAC during AVNRT. During AVNRT, an early PAC can lead to simultaneous fast pathway and slow pathway conduction. At least two conditions are required for this phenomenon to occur: (1) the fast pathway effective refractory period is short enough for the anterograde conduction; and (2) the slow pathway antegrade conduction is delayed enough to exceed the refractoriness of the distal tissue [5]. As a result, the immediate His is advanced by the early PAC via the fast pathway, and tachycardia will continue via the anterograde slow pathway. Although we did not introduce an early PAC to identify a dual atrioventricular nodal response during tachycardia, no dual atrioventricular response, such as during extrastimulus atrial pacing, was observed during sinus rhythm. On the other hand, His-refractory PACs reset the tachycardia and advanced the next His, confirming the diagnosis of AVNRT.
Conclusions
Frequent spontaneous PACs during episodes of AVNRT can be misleading on a surface ECG because of the slightly varying RR intervals. When spontaneous PACs perturb and maintain the AVNRT, their occurrence during His refractoriness is worthy of attention. Endocardial documentation of this timely PAC’s effect on the next His activation is a clue to a positive diagnosis of typical AVNRT for an ongoing tachycardia.
Disclosure statement
AMS has received educational grants from Abbott, Biosense Webster, Biotronik, Boston Scientific and Medtronic through his institution. He received educational grants / lecture honoraria from Bayer, BMS-Pfizer and Daiichi-Sankyo.
Correspondence
Fu Guan, MD
Arrhythmia and Electrophysiology Division
Department of Cardiology
University Heart Centre Zurich
Raemistrasse 100
CH-8091 Zurich
References
1. Diagnostic value of tachycardia features and pacing maneuvers during paroxysmal supraventricular tachycardia. J Am Coll Cardiol. 2000 Aug;36(2):574–82. http://dx.doi.org/10.1016/S0735-1097(00)00770-1PubMed 0735-1097
2. Differentiation of atypical atrioventricular node re-entrant tachycardia from orthodromic reciprocating tachycardia using a septal accessory pathway by the response to ventricular pacing. J Am Coll Cardiol. 2001 Oct;38(4):1163–7. http://dx.doi.org/10.1016/S0735-1097(01)01480-2PubMed 0735-1097
3. . Novel use of atrial overdrive pacing to rapidly differentiate junctional tachycardia from atrioventricular nodal reentrant tachycardia. Heart Rhythm. 2011 Jun;8(6):840–4. http://dx.doi.org/10.1016/j.hrthm.2011.01.011PubMed 1547-5271
4. . Differentiating junctional tachycardia and atrioventricular node re-entry tachycardia based on response to atrial extrastimulus pacing. J Am Coll Cardiol. 2008 Nov;52(21):1711–7. http://dx.doi.org/10.1016/j.jacc.2008.08.030PubMed 0735-1097
5. Influence of ventriculoatrial timing on hemodynamics and symptoms during supraventricular tachycardia. J Cardiovasc Electrophysiol. 2009 Feb;20(2):176–81. http://dx.doi.org/10.1111/j.1540-8167.2008.01276.xPubMed 1045-3873
6. Mechanism of interpretation of two-for-one response to premature atrial complexes during atrioventricular node re-entry tachycardia. Europace. 2020;00:1–6.1099-5129