The authors present the first case of implantation of a novel single-chamber leadless pacemaker capable of atrioventricular (AV) synchronous pacing in a patient with COVID-19 and complete AV block.
Case report
We present the first case of implantation of a novel single-chamber leadless pacemaker capable of atrioventricular (AV) synchronous pacing in a patient with COVID-19 and complete AV block. This device not only promotes AV synchrony, but also eliminates risk of iatrogenic pneumothorax and pocket complications, such as haematoma and infection, and may therefore be considered a valuable alternative to a conventional dual-chamber pacemaker.
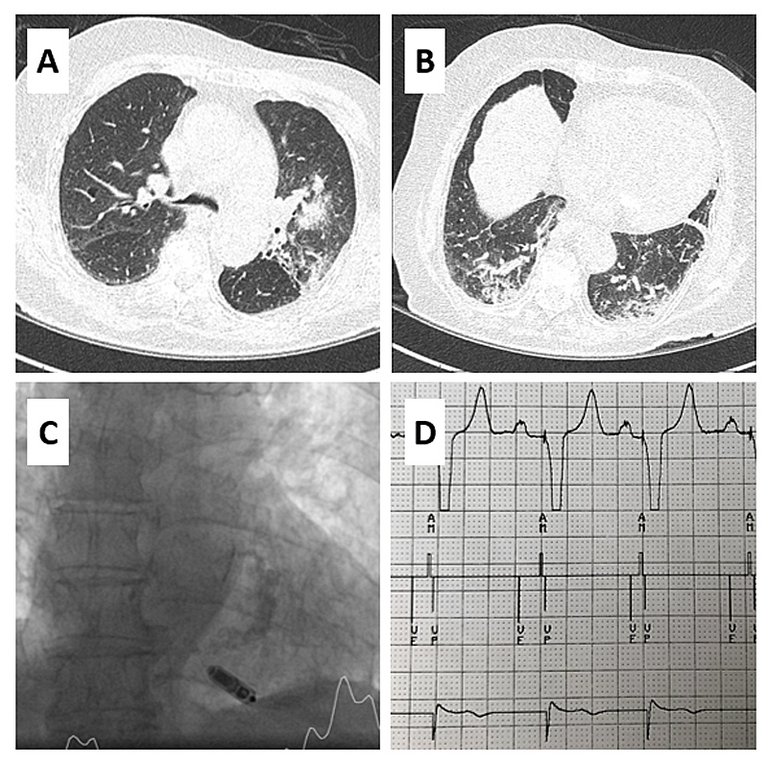
A 90-year-old patient was referred to the emergency department because of progressive fatigue and fever (38°C). The electrocardiogram showed complete atrioventricular (AV) block. The testing for SARS-CoV-2 (severe acute respiratory syndrome coronavirus-2) indicated COVID-19 (coronavirus disease-19). Thoracic computed tomography (CT) showed severe bilateral pneumonia (fig. 1, panels A and B). The clinical and respiratory condition slowly improved but complete AV block persisted. An AV synchronous pacing device with a single-chamber leadless pacemaker (MicraÔ AV, Medtronic, Minneapolis, USA) was successfully implanted 10 days after admission (fig. 1, panel C) and a post-implant electrocardiogram showed AV synchronous pacing (fig. 1, panel D).
Figure 1
Panels A and B show thoracic computed tomography where a bilateral pneumonia due to COVID-19 can be seen. Panel C shows the intra-procedural fluoroscopy image, where the implanted single-chamber pacemaker can be seen. Panel D shows the results of the first pacemaker interrogation after pacemaker implantation. On top is shown the lead II of the surface ECG, in the middle the pacemaker annotations, with the ventricular electogram on the bottom. VE = ventricular end, indicating end of ventricular contraction; AM = atrial mechanical, indicating atrial contraction; both parameters are registered via the pacemaker accelerometer. VP = ventricular pacing .
Although the underlying pathophysiology has remained elusive, various single-centre studies and surveys around the world have reported a spectrum of arrhythmias associated with COVID-19, including AV heart block [1]. Implantation of a conventional pacemaker is the treatment of choice in patients with symptomatic complete AV block, but is associated with a risk of iatrogenic pneumothorax in up to 1.9% of patients, occurring most frequently in old, frail and female patients, as was our patient. Furthermore, because of a disease-related hypercoagulable state, the majority of patients with COVID-19 are anticoagulated [2]. The therapeutic use of heparin carries an increased risk of pocket bleeding, possibly leading to pocket infection.
A leadless intracardiac transcatheter pacing system has been designed to avoid the need for a pacemaker pocket and transvenous leads, and related complications. The long-term safety of the device has recently been reported, with a 48% reduction in the risk of major complications at 12 months compared with a historical control group of patients with transvenous systems, resulting in 82% fewer system revisions and 47% fewer hospitalisations [3]. The MicraÔ leadless pacemaker has progressed from a single-chamber pacemaker that can deliver VVI(R) pacing to a pacing device that can provide AV synchrony via a unique pacing algorithm that relies on identifying mechanical atrial contraction. The performance of this new device has been successfully demonstrated in 75 patients with sinus rhythm and AV block [4].
To the best of our knowledge, this is the first case of implantation of a novel AV leadless pacemaker in a COVID-19 patient; the device may be considered a reasonable alternative to conventional pacemakers in order to avoid perioperative complications including pneumothorax and pocket haematoma/infection, especially in fragile, elderly patients with acute COVID-19.
Disclosure statement
A.A. is a consultant to Boston Scientific, Cairdac, Corvia, Microport CRM, EPD Philips, Radcliffe Publisher. He received speaker fees from Boston Scientific, Medtronic, and Microport. He participates in clinical trials sponsored by Boston Scientific, Medtronic, EPD-Philips. He has intellectual properties with Boston Scientific, Biosense Webster, and Microport CRM. G.C. has received a research grant (PZ00P3_180055) from the Swiss National Science Foundation (SNSF).