A 46-year-old male smoker, with a positive family history of premature coronary artery disease and a history of arterial hypertension and hyperlipidaemia was referred for coronary angiography because of episodes of stabbing precordial chest pain elicited by psychological stress and dyspnoea for the last 2 months. Serial electrocardiograms showed no signs of ischaemia and cardiac enzymes remained within normal limits. Transthoracic echocardiography was notable for suspected hypokinesia of the basal and mid inferior wall. Right transradial coronary angiography demonstrated widespread mild atheromatosis and suspected myocardial bridging of the mid left anterior descending artery. Scrutiny of the angiogram revealed a redundant course of a 5 Fr Judkins left 3.5 diagnostic catheter, which entered the aortic arch after it had formed a high-degree angulation at the right subclavian artery (SCA)-aortic arch junction. In a left anterior oblique caudal view, the peculiar catheter course resembled a slanted letter “Z” (fig. 1a). What do you suspect and what would you do next?
The redundant “Z-like” course of the Judkins left 3.5 catheter made us consider the possibility of an aberrant right SCA or arteria lusoria (AL). Targeted patient interrogation revealed that he had been experiencing dysphagia to solid foods and acid reflux symptoms for about 1 year. Subsequent multislice computed tomography (CT) angiography revealed an AL originating as the last branch of the aortic arch from a position located posterior and to the left of the origin of the left SCA, whereas the right and left carotid arteries were shown to arise from a common trunk (truncus bicaroticus) (fig.1b; electronic supplementary material, video 1). Aneurysmal dilation of the proximal portion or the aortic origin of AL that would have been compatible with a Kommerell diverticulum was not shown. AL followed a retro-oesophageal course with evidence of oesophageal compression (fig. 1c). Our patient was referred for gastroenterological evaluation. Surgical vascular reconstruction should be considered in case of worsening dysphagia despite conservative measures.
Aberrant right SCA or AL constitutes the most common aortic arch anomaly, with an incidence varying from 0.5% to 2.5% [1]. The anomaly is mostly asymptomatic, but in approximately 1 out of 10 cases it usually manifests by compressing the oesophagus and trachea resulting in dysphagia, dyspnoea, retrosternal pain and chronic cough [1, 2]. Dysphagia due to a retro-oesophageal aberrant right SCA compressing the oesophagus is known as dysphagia lusoria. The combination of AL and a bicarotid trunk has an incidence of less than 0.7%, and the presence of a common carotid trunk (truncus bicaroticus) has been reported to predispose to tracheal-oesophageal compression and development of symptoms by impeding the anterior displacement of trachea in the setting of an oesophagus dorsally compressed by AL [1–3]. The presence of AL poses technical challenges during right transradial cardiac catheterisation, thereby reducing the success of the procedure by 40% and increasing the risk of iatrogenic complications such as intramural haematoma or dissection of the artery itself, which may extend to the adjacent aorta [4–6]. Accessing the ascending aorta through the right transradial approach is made difficult in the presence of AL and the catheter tends to advance in the descending aorta. AL traverses through a wider angle at its junction with the aortic arch or the proximal descending aorta and requires the catheter to curve back in order to enter the ascending aorta, leading to certain acquired loops [7]. In our case, the operator did not have unusual difficulty in accessing the ascending aorta, which was achieved with counter-clockwise rotation and then advancement of a Judkins right 4.0 diagnostic catheter over a 0.032-inch guidewire during deep inspiration breath-hold. The latter is a commonly applied manoeuvre that results in downward movement of the aortic root and arch, thereby rendering the angle at the site of origin of the right SCA less wide. Currently, increasingly numbers of patients likely to have dilation and distortion of the aortic root, ascending aorta and aortic arch due to conditions such as long-standing arterial hypertension, severe aortic valve stenosis and chronic aortic regurgitation that simulate AL owing to changes in the anatomy, particularly distances of the origin of the aortic arch branches, undergo right transradial cardiac catheterisation. However, our patient did not have any of the conditions predisposing to pseudo-AL. Therefore, the peculiar “Z-like” course of a Judkins left catheter made us suspect AL. Obtaining a history after angiography with the aim of revealing symptoms that could be caused by AL further strengthened our suspicion.
This case highlights, the importance of taking a complete history that facilitates a proper decision-making process on the need for conventional coronary angiography in patients presenting with chest pain, or the need for other investigations in the case of suspected clinical entities not related to the coronary arteries that could simulate ischaemic heart disease. If a thorough history had been taken in our case from the beginning, we would have diagnosed dysphagia earlier and our patient, who had an intermediate pretest probability of obstructive coronary artery disease, could have been investigated via a different pathway. The latter could involve evaluation by a gastroenterologist in the first place, followed by CT coronary angiography, thereby avoiding conventional coronary angiography, which is an inherently riskier procedure. CT coronary angiography could have been combined with CT angiography of the thoracic aorta and its branches, since AL would have very likely been suspected during the dysphagia workup, specifically by the demonstration of oesophageal compression on barium oesophagography. Furthermore, since AL may simulate ischaemic heart disease, it should be considered in the differential diagnosis of chest pain and the suspicion should be strengthened if the patient also complains of dysphagia. This way, if the patient were to be subjected to conventional coronary angiography, the operator would remain vigilant so as not to miss angiographic signs favouring AL. As highlighted herein, paying attention to the course of the catheters during right transradial coronary angiography is important to suspect and diagnose AL, which might not necessarily cause extreme difficulty in accessing the ascending aorta or be extremely tortuous.
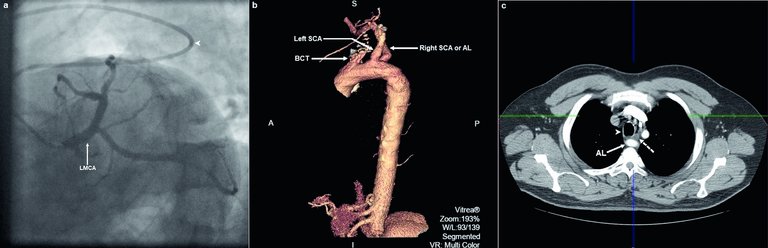
Figure 1:
Conventional invasive coronary and computed tomographic angiographic images. a. Selective left coronary artery angiogram in the left anterior oblique caudal projection. Note, the Judkins left catheter angulation (arrowhead) just before the junction of arteria lusoria (AL) with the aortic arch where it traverses through a wider angle and curves back in order to enter the aortic arch and ascending aorta. Note, also that the course of the catheter from the proximal segment of AL up to the ostium of the left main coronary artery (LMCA) resembles a slanted letter “Z”. b. Three-dimensional volume-rendered reconstruction of aortic multislice computed tomography (MSCT) angiography depicting a left aortic arch and an aberrant right subclavian artery (SCA) or AL originating distal to the origin the left SCA. A common trunk of right and left common carotid arteries (BCT; bicarotid trunk) is displayed as the first branch of the aortic arch. c. Axial multiplanar reconstruction of aortic MSCT angiography depicting the oesophagus (dotted arrow) that is compressed between the trachea (arrowhead) and the dorsally located AL (solid arrow).
2. . The aberrant right subclavian artery (arteria lusoria): the morphological and clinical aspects of one of the most important variations—a systematic study of 141 reports. ScientificWorldJournal. 2014;2014:292734. http://dx.doi.org/10.1155/2014/292734PubMed
6. . Dissection of Arteria Lusoria during Transradial PCI: A Rare Complication revealed and followed by Multidetector CT. J Cardiol Ther. 2013;1:34–6. http://dx.doi.org/10.12970/2311-052X.2013.01.02.1
7. . The problem of arteria lusoria in right transradial coronary angiography and angioplasty. Catheter Cardiovasc Interv. 2001 Oct;54(2):196–201. http://dx.doi.org/10.1002/ccd.1266PubMed