All echocardiographic evidence of bioprosthesis thrombosis disappeared during the 48 hours of intravenous treatment with unfractionated heparin.
Case description
A 62-year-old male patient was urgently referred to our hospital by his attending cardiologist owing to a large hypermobile mass on his mitral valve bioprosthesis that was detected during routine echocardiographic follow-up. The patient presented in good general condition and had no worsening of cardiac symptoms, or any clinical signs of cardiac decompensation. His current daily medication consisted of rivaroxaban 20 mg, metoprolol 100 mg, lisinopril 20 mg and torasemide 5 mg.
His past medical history included mitral valve replacement with a mechanical prosthesis in 1999 for severe mitral regurgitation. In 2011, pulmonary vein isolation was performed for atrial fibrillation. This procedure was followed by three electrical cardioversion therapies after recurrence of atrial fibrillation in 2011 and 2012. During this time period, systolic heart failure with a left ventricular ejection fraction of 30% was diagnosed. In 2017, an emergency repeat mitral valve replacement with a biological valve (CE Edwards, Perimount Magna Ease 31mm bioprosthesis) had to be performed because of mechanical prosthesis thrombosis leading to haemodynamic instability. At that time, the patient was non-compliant with his medication, having stopped phenprocoumon intake for many weeks prior to this life-threatening event. Subsequently, after having received a mitral bioprosthetic valve, oral anticoagulation was changed to rivaroxaban 20 mg daily. Five months prior to the current presentation his cardiac examination showed normal sinus rhythm, a left ventricular ejection fraction of 28% and normal mitral bioprosthesis function.
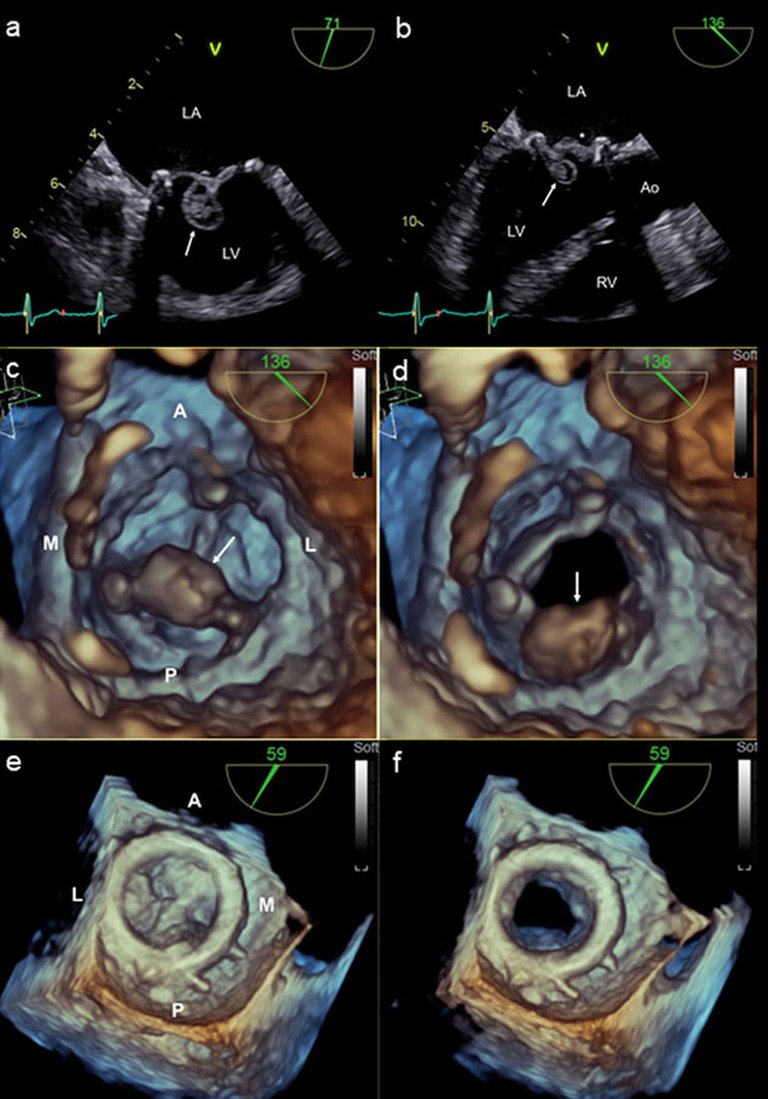
On admission to our hospital, a transoesophageal echocardiogram was performed. This examination confirmed the presence of a large hypermobile mass attached to the ventricular side of the bioprosthesis (fig. 1a–d). The mass was 1.5 cm in diameter and appeared to have solid as well as echo-lucent aspects. Additionally, diffuse thickening of the prosthetic cusps was detected (fig. 1b, e). On three-dimensional (3D) images, the surface of the atrial aspect of the cusps could not be sharply delineated (fig. 1e) and on ventricular views, the large roundish mass was attached to the posterior cusp (fig. 1c, d). Valve opening was not relevantly impaired (fig. 1d, f) and there was no regurgitation (colour Doppler images not shown).
Figure 1
Echocardiographic grey scale (a,b) and 3D images (c–f) before intravenous treatment with unfractionated heparin. A large mass 1.5 cm in diameter is located at the ventricular side of the mitral valve bioprosthesis (arrow, a–d). The mass appears to have solid aspects as well as liquid inclusions (a, b) and is attached to the posterior cusp (c,d). The other cusps are diffusely thickened (asterix, b) and from the atrial aspect, the single cusps cannot be sharply delineated in closed position (e). Valve opening is not relevantly impaired (d, f). LV = left ventricle; LA = left atrium; RV = right ventricle; Ao = ascending aorta; A = anterior; L = lateral; P = posterior; M = medial.
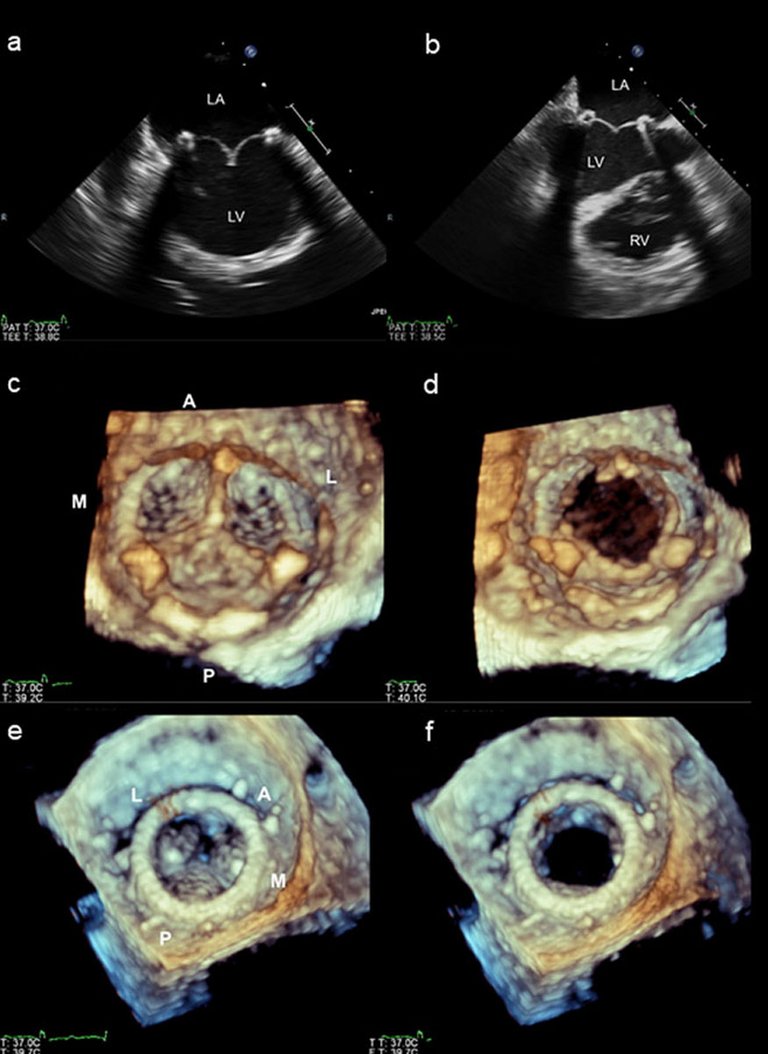
There were no clinical signs of infective disease and inflammatory laboratory parameters were within normal limits, making the diagnosis of an infectious endocarditis very unlikely. Based on our findings, we suspected the presence of bioprosthetic valve thrombosis comprising a large spherical hypermobile mass and diffuse prosthesis thrombosis resulting in diffuse cusp thickening. Of note, these findings occurred despite treatment with rivaroxaban, which the patient claimed to have taken regularly without interruption. Treatment with intravenous unfractionated heparin was initiated and after discussion in our heart team, the decision was made to perform “re-re-do” mitral valve replacement the day after next. On the day of the scheduled operation, the transoesophageal echocardiogram performed during initiation of surgery could no longer detect the thrombotic mass previously present on the ventricular aspect of the posterior prosthetic cusp (fig. 2). Surprisingly, not only the round mass had disappeared from the bioprosthetic valve (fig. 2a–d), but the diffuse cusp thickening had also vanished, resulting in thin cusps (fig. 2a, b) whose atrial surface became more clearly distinguishable on 3D images (fig. 2e). Since the appearance of the bioprosthetic valve had virtually normalised and valve function was preserved, surgery was cancelled. The patient remained on treatment with intravenous unfractionated heparin and, subsequently, oral anticoagulation with phenprocoumon was initiated. During the course of the hospitalisation, no clinical evidence of an embolic event was observed. Also, there were no signs of renal, hepatic or intestinal dysfunction. An echocardiographic follow-up performed two months later showed normal function of the mitral bioprosthesis with no evidence of thrombus recurrence.
Figure 2
Echocardiographic grey scale (a,b) and 3D images (c–f) performed after less than 48 hours of treatment with intravenous unfractionated heparin. The hypermobile mass can no longer be visualised (a–d). The single cusps are thin (a,b) and, compared to the situation before heparin therapy, their surface and borders can be better delineated from the atrial view (e). LV = left ventricle; LA = left atrium; RV = right ventricle; A = anterior; L = lateral; P = posterior; M = medial.
Discussion
Bioprosthetic valve thrombosis is a potentially life-threatening complication. The risk of thromboembolism related to bioprostheses is thought to be low after the initial three months post-implantation [1]. However, bioprosthetic valve thrombosis may also occur late after implantation. In one study, the peak incidence of thrombosis was 13–24 months after surgery [2].
The reported incidence of clinically overt bioprosthetic valve thrombosis varies widely. In the mitral position, a rate of up to 6% has been stated in literature [3]. According to computed tomographic registries, subclinical bioprosthesis thrombosis may occur in as many as 13% of transcatheter and 4% of surgically implanted aortic bioprostheses [4]. Corresponding data for the incidence of subclinical bioprosthesis thrombosis in the mitral position are not available.
In our patient, valve thrombosis occurred 52 months after “re-do” mitral valve replacement. Despite extensive thrombosis with diffuse cusp thickening and formation of a large mass on the valve surface, no relevant prosthesis dysfunction was found.
In the mitral position, bioprosthesis thrombosis is usually located at the atrial side of the prosthesis [1]. This was different in our patient, who exhibited a large hypermobile mass on the ventricular aspect of the valve.
In accordance with the principles of the Virchow´s triad, three main mechanisms are responsible for endovascular thrombus formation: the surface factor, the haemodynamic factor and the haemostatic factor [5, 6].
Unlike the normal endothelium, the surface of prosthetic valves, as an artificial material, has a propensity for clotting. After three months, the surface of an implanted bioprosthesis is covered by a neointimal layer composed of smooth muscle cells, extracellular matrix and endothelial cells [7]. Incomplete prosthesis endothelialisation may be one factor leading to vulnerability of a bioprosthesis to thrombus apposition. Other potential reasons for surface activation might be leaflet damage or prosthetic stent fracture [5]. In our case, after administration of intravenous heparin, the valve showed a normal appearance with no apparent signs of cusp damage or other forms of prosthesis deterioration.
Haemodynamic factors related to prosthesis thrombosis include low cardiac output, prosthesis malposition and the prosthesis-specific haemodynamic profile [5]. In our patient, reduced left ventricular ejection fraction, paroxysmal atrial fibrillation and left atrial dilatation may have accounted for slow blood flow across the valve. Moreover, as a result of differences in the haemodynamic profile, the stented design of the implanted bioprosthesis may be related to a somewhat higher risk of thrombosis compared with stentless prostheses [8].
The third mechanism is the haemostatic factor related to primary or secondary hypercoagulable states [5]. Haematological assessment did not reveal evidence for the presence of a coagulopathy in our patient. Among others, antiphospholipid syndrome and antithrombin III deficiency were excluded. Moreover, there were no signs of a myeloproliferative disorder or findings suggestive of presence of a paraneoplastic state.
Oral anticoagulation, both with warfarin as well as with novel oral anticoagulants (NOAC), is thought to be effective in prevention of subclinical leaflet thrombosis [4]. Our patient was kept on long-term treatment with rivaroxaban for atrial fibrillation. However, this regimen was not able to prevent formation of a large thrombus on his mitral bioprosthetic valve. The patient declared credibly that he had taken his medication on a daily basis. We did not test for anti-factor Xa activity on admission. However, the international normalised ratio (INR) was elevated at 1.53 and the thrombophilia laboratory work-up showed evidence of anti-factor Xa activity. Although not clear proof, these findings support his adherence to the NOAC medication.
In haemodynamically stable patients with bioprosthesis thrombosis, guidelines first recommend optimisation of anticoagulation, monitoring for thromboembolism and echocardiographic follow-up before considering re-intervention [9]. In the absence of a very high risk for prosthesis obstruction or potentially fatal thromboembolism, a “wait-and-see” strategy should thus be followed. This may be particularly true if a “re-re-do” surgical procedure is planned. However, the risk of embolisation of the large hypermobile thrombus and its potentially grave clinical consequences led to the team decision to schedule the patient for urgent surgery. After a period of less than 48 hours of treatment with intravenous unfractionated heparin, not only had the large spherical thrombus disappeared from the prosthesis, but to our surprise, this short period of intravenous anticoagulation also led to complete reversion of diffuse cusp thickening, indicating rapid vanishing of diffuse prosthesis thrombosis.
Correspondence
Lixi Caspary, MD, Department of Cardiology, Stadtspital Triemli, Birmensdorferstrasse 497, CH-8063 Zurich, Lixi.Caspary[at]triemli.zuerich.ch
2Pislaru SV, Hussain I, Pellikka PA, Maleszewski JJ, Hanna RD, Schaff HV, et al.Misconceptions, diagnostic challenges and treatment opportunities in bioprosthetic valve thrombosis: lessons from a case series. Eur J Cardiothorac Surg. 2015;47(4):725–32. doi:. http://dx.doi.org/10.1093/ejcts/ezu201PubMed
3Butnaru A, Shaheen J, Tzivoni D, Tauber R, Bitran D, Silberman S. Diagnosis and treatment of early bioprosthetic malfunction in the mitral valve position due to thrombus formation. Am J Cardiol. 2013;112(9):1439–44. doi:. http://dx.doi.org/10.1016/j.amjcard.2013.06.014PubMed
4Chakravarty T, Søndergaard L, Friedman J, De Backer O, Berman D, Kofoed KF, et al.; RESOLVE; SAVORY Investigators. Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study. Lancet. 2017;389(10087):2383–92. doi:. http://dx.doi.org/10.1016/S0140-6736(17)30757-2PubMed
6Wolberg AS, Aleman MM, Leiderman K, Machlus KR. Procoagulant activity in hemostasis and thrombosis: Virchow’s triad revisited. Anesth Analg. 2012;114(2):275–85. doi:. http://dx.doi.org/10.1213/ANE.0b013e31823a088cPubMed
7Noble S, Asgar A, Cartier R, Virmani R, Bonan R. Anatomo-pathological analysis after CoreValve Revalving system implantation. EuroIntervention. 2009;5(1):78–85. doi:. http://dx.doi.org/10.4244/EIJV5I1A12PubMed
8Sun JC, Davidson MJ, Lamy A, Eikelboom JW. Antithrombotic management of patients with prosthetic heart valves: current evidence and future trends. Lancet. 2009;374(9689):565–76. doi:. http://dx.doi.org/10.1016/S0140-6736(09)60780-7PubMed
9Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al.; ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739–91. doi:. http://dx.doi.org/10.1093/eurheartj/ehx391PubMed