A 54-year-old male patient was brought to the emergency department with palpitations, dizziness and shortness of breath late on a Friday evening. He had a history of palpitations for a few years, but no other past medical history. The 12-lead ECG revealed a very fast wide-complex tachycardia (WCT) of 250 bpm (fig. 1). Because of haemodynamic instability with a blood pressure of 50/30 mm Hg, direct-current cardioversion was performed and restored sinus rhythm (fig. 2) with resolution of symptoms. The patient was admitted to the intermediate care unit for surveillance. After a few hours, another, but slower, WCT started (fig. 3). This was haemodynamically stable at first, but soon degenerated into atrial fibrillation with a very rapid ventricular response, requiring cardioversion again. Over the course of the subsequent 48 hours, the fast WCT recurred repeatedly with heart rates above 200 bpm (often irregular) despite initiation of amiodarone, beta blocker and calcium channel blocker therapy. Multiple direct-current cardioversions were performed but could not prevent development of progressive cardiogenic shock with multiorgan failure.
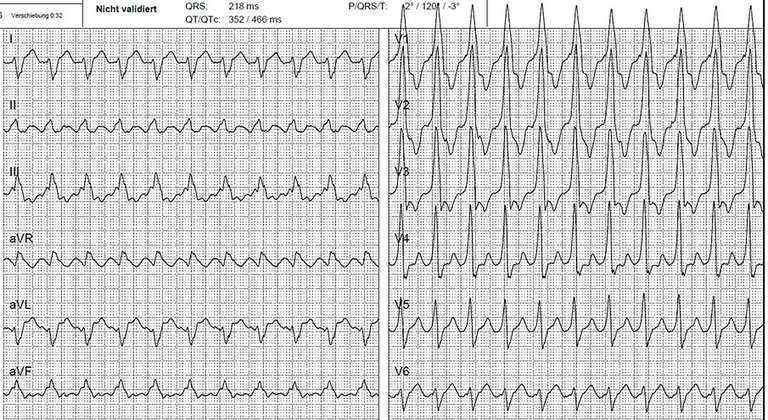
Figure 1
ECG on admission.
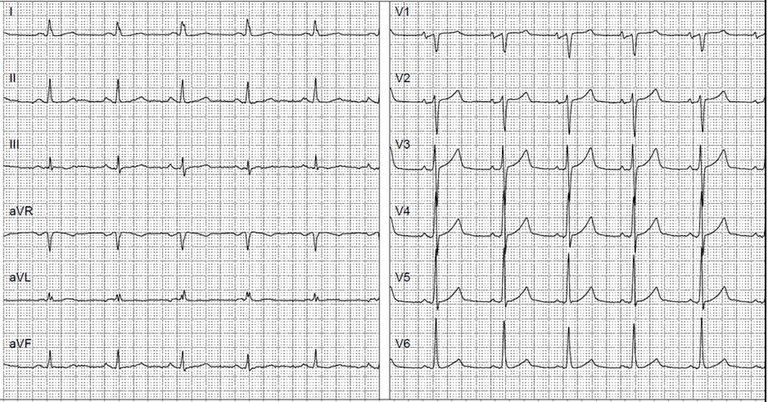
Figure 2
ECG after cardioversion.
Figure 3
ECG on recurrence of the wide-complex tachycardia.
What is your diagnosis and what are the next steps in the management of this patient?
Despite the absence of a cardiac past medical history, the initial very fast WCT (fig. 1) was highly suggestive of ventricular tachycardia (VT). Both the Brugada and the lead aVR algorithm classified the WCT as VT [1, 2]. The sinus rhythm ECG after direct-current cardioversion did not show ST-elevations indicative of a ST elevation myocardial infarction (STEMI) as the cause of the VT (fig. 2). There was no obvious delta wave as an indicator for an antegradely conducting accessory pathway (AP) causing an antidromic atrioventricular reentrant tachycardia. At first recurrence of the WCT, the 12-lead ECG showed atrial flutter with 2:1 conduction (fig. 3). The heart rate (125 bpm) was exactly half of the initial heart rate and the QRS morphology was the same as that on the initial ECG. This was no longer compatible with a diagnosis of VT. At this point, the working hypothesis was atrial flutter with aberrancy in the right bundle branch and in the left posterior fascicle, and an initial 1:1 and later 2:1 conduction to the ventricles. This hypothesis was, however, challenged by the clinical course with heart rates persistently over 200 bpm (in both atrial flutter and atrial fibrillation) despite the initiation of several atrioventricular-node-blocking medications.
In an electrophysiology study conducted after the weekend, atrial pacing revealed the presence of a left sided AP, which was successfully ablated by retrograde aortic approach due to a thrombus in the left atrial appendage detected on transoesophageal echocardiography. Cavotricuspid isthmus ablation was performed in the same session. The sinus rhythm ECG after ablation is shown in figure 4. The patient recovered with no residues. On follow-up 2 months after ablation, there was no evidence for AP recovery, but Holter monitoring revealed asymptomatic paroxysmal atrial fibrillation.
Figure 4
ECG after accessory pathway ablation.
Discussion
Preexcitation reflected by a shortened PR interval and presence of a delta wave is the ECG hallmark of antegradely conducting APs. The degree of preexcitation varies with AP location and conduction properties. It is generally more remarkable with right sided than with left sided APs because of the time needed for intra- and interatrial conduction between the sinus node and the atrial insertion of the AP. Criteria suggested to indicate ventricular preexcitation in ambiguous situations include the absence of septal q-waves in V6 or of septal r-waves in aVR [3, 4]. In our patient, both septal q-wave and septal r-wave were present in the sinus rhythm ECG (fig. 2) and according to these criteria should have indicated the absence of preexcitation. However, the R/S transition <V1 during sinus rhythm should prompt the clinician to think about the possibility of a left sided AP.
Preexcitation may be subtle or even absent with slow heart rates, but it becomes more easily apparent with faster heart rates. This was the case in our patient both during his clinical tachycardia episodes when the atrial flutter was conducting through the AP 1:1 or 2:1 and during atrial pacing in the electrophysiology study. The QRS morphology with right bundle branch block in V1 and a right-inferior axis in the extremity leads was clearly indicative of an anterolateral left sided AP.
Although the elimination of AP conduction by means of catheter ablation is curative, this approach is not always immediately available (e.g., on weekends). In such situations, medical treatment may be needed as a bridge to ablation in cases with recurrent, preexcited supraventricular tachycardias. Both atrioventricular-node-blocking agents and amiodarone should be avoided because they may increase the risk of ventricular fibrillation; however, class Ic antiarrhythmic drugs such as flecainide or propafenone can be used to slow AP conduction and should have been the drugs of choice in our case [5].
Patients with atrioventricular APs have an increased risk of up to 30% for developing atrial fibrillation [5], which can organise to atrial flutter. Successful AP ablation may substantially reduce the risk for subsequent atrial fibrillation (and potentially atrial flutter), particularly in patients younger than 50 years (12% recurrent AF over 2 years), but not so much in patients older than 50 years (35% recurrent atrial fibrillation over 2 patient was 54 years old and atrial flutter with 1:1 conduction over the AP was the years) [6, 7]. Our clinical arrhythmia leading to cardiogenic shock. Accordingly, we decided to perform cavotricuspid isthmus ablation in addition to AP ablation to avoid a similar situation by all means.
In summary, the uncommon combination of two common things, atrial flutter and a left lateral AP, led to recurrent episodes of preexcited atrial flutter and atrial fibrillation. The presence of just minimal preexcitation in the 12-lead ECG during slow sinus rhythm made the correct diagnosis challenging and delayed appropriate treatment.
Correspondence
Prof. Tobias Reichlin, MD, FESC, Department of Cardiology, Inselspital, Bern University Hospital, University of Bern, Freiburgstrasse 18, CH-3010 Bern,, tobias.reichlin[at]insel.ch
References
1Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991;83(5):1649–59. doi:. http://dx.doi.org/10.1161/01.CIR.83.5.1649PubMed
2Vereckei A, Duray G, Szénási G, Altemose GT, Miller JM. New algorithm using only lead aVR for differential diagnosis of wide QRS complex tachycardia. Heart Rhythm. 2008;5(1):89–98. doi:. http://dx.doi.org/10.1016/j.hrthm.2007.09.020PubMed
3Bogun F, Kalusche D, Li YG, Auth-Eisernitz S, Grönefeld G, Hohnloser SH. Septal Q waves in surface electrocardiographic lead V6 exclude minimal ventricular preexcitation. Am J Cardiol. 1999;84(1):101–4, A9. doi:. http://dx.doi.org/10.1016/S0002-9149(99)00203-9PubMed
4Eisenberger M, Davidson NC, Todd DM, Garratt CJ, Fitzpatrick AP. A new approach to confirming or excluding ventricular pre-excitation on a 12-lead ECG. Europace. 2010;12(1):119–23. doi:. http://dx.doi.org/10.1093/europace/eup345PubMed
5Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomström-Lundqvist C, et al.; ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020;41(5):655–720. doi:. http://dx.doi.org/10.1093/eurheartj/ehz467PubMed
6Schwieler JH, Zlochiver S, Pandit SV, Berenfeld O, Jalife J, Bergfeldt L. Reentry in an accessory atrioventricular pathway as a trigger for atrial fibrillation initiation in manifest Wolff-Parkinson-White syndrome: a matter of reflection?Heart Rhythm. 2008;5(9):1238–47. doi:. http://dx.doi.org/10.1016/j.hrthm.2008.05.028PubMed
7Dagres N, Clague JR, Lottkamp H, Hindricks G, Breithardt G, Borggrefe M. Impact of radiofrequency catheter ablation of accessory pathways on the frequency of atrial fibrillation during long-term follow-up; high recurrence rate of atrial fibrillation in patients older than 50 years of age. Eur Heart J. 2001;22(5):423–7. doi:. http://dx.doi.org/10.1053/euhj.2000.2429PubMed