Syncope is defined as a transient loss of consciousness due to cerebral hypoperfusion, characterised by a rapid onset, short duration and spontaneous complete recovery [1]. Syncope has a large differential diagnosis, is difficult to evaluate and can be disabling. The presence of heart disease is a crucial factor in prognosis and risk stratification, hence the importance of identifying syncope of cardiac origin.
Elpidoforos et al. evaluated the incidence, specific causes, and prognosis of syncope in the Framingham Heart Study. The incidence of syncope of cardiac origin was 9.5% [2], which means that a considerable number of patients are exposed to a significant risk of sudden cardiac death.
History, physical examination, blood pressure and ECG help in the initial evaluation of a patient presenting with syncope, and Holter monitoring, and R-test and loop recorders help further in investigating those at high risk for a cardiac origin. New noninvasive devices have been introduced in recent years (table 1), but none of them have become widespread diagnostic tools in the ambulatory setting, even though their development is very promising.
Case report
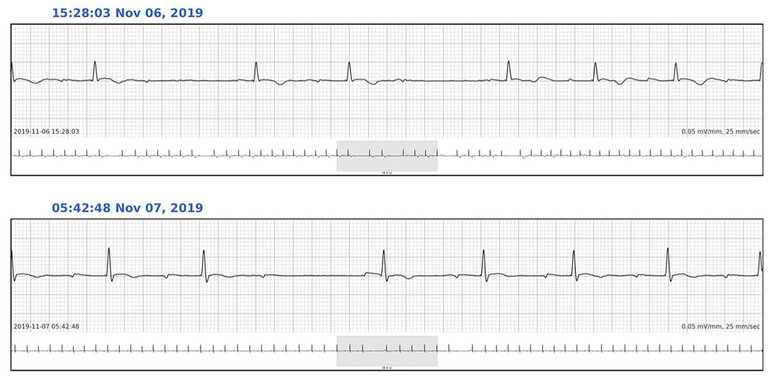
A 33-year-old otherwise healthy woman was referred to our cardiology clinic for syncope and palpitations. She reported having palpitations for 3 months. The palpitations were described as regular and strong, happening mainly at rest in the evening. The syncope occurred when she came back home after horse riding in the late afternoon. She experienced sudden palpitations with perspiration and dizziness before lying down and losing consciousness. The patient felt that the loss of consciousness was complete and very brief. No one witnessed the event. She denied any chest pain, or dyspnoea. The recovery was prompt and complete. The clinical examination was unremarkable except for low blood pressure (97/64 mm Hg). Transthoracic echocardiography was normal. A 12-lead ECG demonstrated first degree atrioventricular (AV) block. A treadmill exercise testing was supramaximal (15 metabolic equivalents [METs]) and could not induce any arrhythmia or ischaemia. Based on this initial investigation, the prognostic scores were uncertain (EGSYS 3 points, OESIL 1 point; see tables 2, 3, 4, 5). Therefore, a handheld ECG was given to the patient together with a 3-day SmartCardia (SmartCardia, EPFL Innovation Park, Lausanne, Switzerland) recorder (fig. 1). Four recordings were performed during palpitations with the handheld ECG and demonstrated normal sinus rhythm. Analysis of the SmartCardia recordings revealed two episodes of second-degree AV block (fig. 2). As a result of this benign finding and after ruling out active Lyme disease and discussing a cardiac electrophysiology study with the patient, only counter-pressure manoeuvres were recommended.
Figure 1
SmartCardia device.
Figure 2
Holter findings. The asterisks (*) indicate second degree atrioventricular block.
Discussion
Currently, two patch-based devices are commercially available (table 1). This case illustrated the possible use of the SmartCardia device in patients who experience palpitation and/or loss of consciousness of unknown cause.
SmartCardia is a versatile patch-based device able to measure many different parameters: single-lead ECG (with automated real-time detection of atrial fibrillation and other arrhythmias, heart rate, heart rate variability), respiration rate (and apnoea-hypopnoea index), oxygen saturation, skin temperature, posture and activity, as well as blood pressure variations.
Moreover, the device offers up to 7 days of data storage and 3-day real-time connectivity through a smartphone. The ability to receive, store and interpret a broad range of parameters offers the opportunity to go far beyond monitoring individual parameters.
The cloud platform allows for multiple patient views, showing the real-time ECG signal and parameters. The cloud platform also makes real-time automated arrhythmia calls, which include bradycardia, tachycardia, atrial fibrillation and pause, based on built-in machine learning models that are validated against patient data manually annotated by cardiologists. Finally, the cloud system allows healthcare professionals to browse all the historical data of the patient, analyse it and generate reports.
SmartCardia is a newly commercialised system but is still under development. Its versatile configuration can offer varied and complete monitoring. We have tested the cardiac monitoring system [8]. In view of its light weight and simplicity of use, the system is valuable. The noise level was low. Nevertheless, because of its single-lead architecture, the reliability and accuracy of the signal compared with conventional Holter monitoring has yet to be demonstrated. In this respect, several comparative studies are currently underway.
EGSYS (Evaluation of Guidelines in SYncope Study) score for syncope [6].
Finding
Points
Abnormal ECG* and/or heart disease**
+3
Palpitations before syncope
+4
Syncope during effort
+3
Syncope in supine position
+2
Autonomic prodromes***
−1
Predisposing and/or precipitating factors****
−1
* Sinus bradycardia, atrioventricular block >1st degree, bundle branch block, acute or old myocardial infarction, supraventricular or ventricular tachycardia, left or right ventricular hypertrophy, ventricular pre-excitation, long QT or Brugada pattern. ** Previous clinical or laboratory diagnosis of any form of structural heart disease, including ischemic heart disease, valvular dysfunction, cardiomyopathies and congenital heart disease; previous diagnosis or clinical evidence of congestive heart failure; physical signs of structural heart disease. *** Nausea/vomiting. **** Warm or crowded place, prolonged orthostasis, fear / pain / other emotion.
Table 3
Interpretation of the EGSYS (Evaluation of Guidelines in SYncope Study) score.
Score
Interpretation
Mortality at 21–24 months
≥3
Cardiac syncope likely (95% sensitive)
17%
<3
Cardiac syncope less likely
3%
Table 4
OESIL (Osservatorio Epidemiologico della Sincope nel Lazio) score for syncope [7].
Item
Points
Age >65 years
+1
Cardiovascular disease in clinical history*
+1
Syncope without prodrome
+1
Abnormal ECG**
+1
* Cardiovascular disease is defined as any of the following: previous clinical or laboratory diagnosis of any form of structural heart disease, including ischaemic heart disease, valvular dysfunction and primary myocardial disease; previous diagnosis or clinical evidence of congestive heart failure; previous diagnosis or clinical evidence of peripheral arterial disease; previous diagnosis of stroke or transient ischaemic attack. ** Abnormal ECG is defined as any of the following: rhythm abnormalities (atrial fibrillation or flutter, supraventricular tachycardia, multifocal atrial tachycardia, frequent or repetitive premature supraventricular or ventricular complexes, sustained or non-sustained ventricular tachycardia, paced rhythms): atrioventricular (AV) or intraventricular conduction disorders (complete AV block, Mobitz I or Mobitz II AV block, bundle branch block, or intraventricular conduction delay); left or right ventricular hypertrophy; left axis deviation; old myocardial infarction; ST segment and T wave abnormalities consistent with or possibly related to myocardial ischemia. Non-specific repolarisation abnormalities are not considered abnormal.
Table 5
Interpretation of the OESIL (Osservatorio Epidemiologico della Sincope nel Lazio) score.
Score
Mortality
0 points
0%
1 point
0.8%
2 points
19.6%
3 points
34.7%
4 points
57.1%
Correspondence
Prof. Stéphane Cook, MD, Cardiology Department, University and Hospital Fribourg, Chemin de Pensionnats 2−6, 1708 Fribourg, Email:stephane.cook[at]unifr.ch
References
1Brignole M, Moya A, de Lange FJ, Deharo J-C, Elliott PM, Fanciulli A, et al.; ESC Scientific Document Group. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39(21):1883–948. doi:. http://dx.doi.org/10.1093/eurheartj/ehy037PubMed
2Soteriades ES, Evans JC, Larson MG, Chen MH, Chen L, Benjamin EJ, et al.Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878–85. doi:. http://dx.doi.org/10.1056/NEJMoa012407PubMed
3Barrett PM, Komatireddy R, Haaser S, Topol S, Sheard J, Encinas J, et al.Comparison of 24-hour Holter monitoring with 14-day novel adhesive patch electrocardiographic monitoring. Am J Med. 2014;127(1):95.e11–7. doi:. http://dx.doi.org/10.1016/j.amjmed.2013.10.003PubMed
4Engel JM, Chakravarthy BLN, Rothwell D, Chavan A. SEEQ™ MCT wearable sensor performance correlated to skin irritation and temperature. Conf Proc IEEE Eng Med Biol Soc. 2015;2015:2030–3. PubMed
5Rho R, Vossler M, Blancher S, Poole JE. Comparison of 2 ambulatory patch ECG monitors: The benefit of the P-wave and signal clarity. Am Heart J. 2018;203:109–17. doi:. http://dx.doi.org/10.1016/j.ahj.2018.03.022PubMed
6Del Rosso A, Ungar A, Maggi R, Giada F, Petix NR, De Santo T, et al.Clinical predictors of cardiac syncope at initial evaluation in patients referred urgently to a general hospital: the EGSYS score. Heart. 2008;94(12):1620–6. doi:. http://dx.doi.org/10.1136/hrt.2008.143123PubMed
7Ammirati F, Colivicchi F, Santini M. Diagnosing syncope in clinical practice. Implementation of a simplified diagnostic algorithm in a multicentre prospective trial - the OESIL 2 study (Osservatorio Epidemiologico della Sincope nel Lazio). Eur Heart J. 2000;21(11):935–40. doi:. http://dx.doi.org/10.1053/euhj.1999.1910PubMed
8Murali S, Rincon F, Cassina T, Ferrari E, Cook S, Goy JJ. Clinical comparison of a new smart wearable wireless rhythm monitoring system with standard ECG monitoring in the ICU: a pilot trial. MIR Biomedical Engineering. 2020; (in production).