François P. Sarasin,
Olivier Hugli,
Juan M. Sztajzel,
Jürg Schläpfer,
Monica Varcher-Herrera,
Johan Graz,
Christophe Berchier,
Corinne Mischler,
Etienne Pruvot
Syncope is a common symptom in emergency department visits and, despite extensive evaluation, still remains unexplained in a significant number of cases.The findings of this study support the concept that patients with SUA suffer from some form of neurally mediated syncope.
Introduction
Syncope is a common symptom, accounting for 1–5% of all emergency department (ED) visits and 1–3% of hospital admissions [1–4]. Guidelines on syncope management recommend performing a careful history, physical examination, electrocardiogram (ECG), supine and standing blood pressure measurements and, in patients over 40 years, a carotid sinus massage [1]. Despite these recommendations, syncope remains of unexplained aetiology (SUA) in 10–60% of the cases in general practice [5–9]. The use of standardised work-ups and specialised syncope facilities improves the diagnostic yield, but syncope still remains unexplained in 5–20% of the cases [10]. The ISSUE study, in which an implantable loop recorder (ILR) was used in SUA patients with a normal ECG, no structural heart disease and a positive or negative tilt-testing, has shown that most recurrences occurred concomitantly with a progressive sinus bradycardia and ventricular asystole [11]. This finding is suggestive of a neurally mediated mechanism regardless of the tilt-table test results.
The present study focused on patients with SUA after a structured a work-up. We hypothesised that SUA is underdiagnosed neurally mediated syncope (NMS), with similar clinical and paraclinical characteristics, and recurrence and death rates.
Methods and statistical analysis
Method
This study was a subanalysis of an investigation conducted from 1 January 2003 to 30 June 2004 in the EDs and the general internal medicine clinics of two primary and tertiary care public hospitals, the Geneva University Hospital (HUG, Hôpitaux Universitaires de Genève, Switzerland) and the Lausanne University Hospital (CHUV, Centre Hospitalier Universitaire Vaudois, Switzerland) [12]. All patients over 18 years admitted in the ED with a chief complaint of syncope were eligible. Syncope was defined as a sudden and transient loss of consciousness with an inability to maintain postural tone, followed by spontaneous recovery. Patients with vertigo, dizziness, symptoms suggesting seizure disorders (prolonged recovery and witnessed sustained tonic-clonic movement), traumatic or alcohol associated altered mental status were excluded [12].
Study design
This study was approved by both institutional ethics committees and the detailed methodology has been previously published [12]. This was a prospective study including two consecutive investigational phases (see fig. 1 below). Phase I occurred from time of arrival to discharge from the ED. Eligible patients underwent a standardised evaluation including careful history, physical examination, 12-lead ECG and measurement of blood pressure in the supine and upright positions. Based on explicit predefined criteria, study investigators classified patients into three groups as follows: (1) patients in whom a cause of syncope was established based on the initial evaluation; (2) patients in whom the aetiology of syncope was suspected during the initial evaluation but required confirmation by targeted diagnostic procedures; and (3) patients with SUA. Patients in the second group with negative targeted tests and those in the third group were asked to participate in the phase II evaluation.
In phase II, in order to minimise the effect of physicians’ increasing experience and contamination of intervention over control periods, patients were allocated alternatively to one of the two periods on a 3-month basis. During the intervention periods, patient’s evaluation was based on a stepwise diagnostic work-up [12]. During the control periods, investigations were left to the discretion of the physicians in charge without intervention from the study investigators.
Patients with dementia, poor health status (such as malignancy, severe stroke) or inability to undergo any diagnostic test were excluded from phase II. In this secondary analysis, we also excluded patients of the control periods in whom the standardised work-up was not systematically applied and those who were lost to follow-up at 12 months.
Intervention group
During the phase II intervention period, the stepwise diagnostic work-up was standardised. Patients with a normal ECG and no history of heart disease were evaluated for NMS only if syncope was recurrent (≥2 episodes) or severe (car accident and/or major trauma) [10]. Tests for NMS included head-up tilt testing and bilateral supine and standing carotid sinus massage [12]. In the presence of heart disease and/or an abnormal ECG (see appendix 1 for definition of an abnormal ECG), the following evaluation included, if indicated, transthoracic echocardiography, 24-hour Holter recording, a cardiac exercise treadmill stress test and a coronary angiogram. Moreover, an electrophysiological study was performed in patients with: (1) previous myocardial infarction with a left ventricular ejection fraction (LVEF) ≤40% or regional wall motion abnormalities; (2) nonischaemic dilated cardiomyopathy and LVEF ≤40%; or (3) ECG or 24-hour Holter recording findings suggestive of sinus node dysfunction or atrioventricular block.
Procedure and data collection
The decision regarding hospital admission was left to the ED physicians, and the selected cardiological examinations were performed by a consultant cardiologist unaware of the study protocol. A dedicated research physician at each site supervised daily patients’ inclusion and completion of data collection.
Diagnostic criteria
The cause for syncope was defined at 30 days according to explicit predefined criteria [12]. If a cause was uncertain, the diagnosis was reached by consensus of a committee of three internists and two cardiologists. If the cause of syncope was identified, the choice of a diagnosis-specific treatment was left to the physician in charge of patient.
Statistical analysis
Continuous variables were compared with analysis of variance (ANOVA) and categorical variables with Fisher’s exact test. For the multiple comparisons between each groups a Bonferroni correction was applied and a p-value <0.0033 was considered statistically significant. Statistical tests were performed using Statview version 5 (SAS Institute Inc., Cary, NC 27513, USA).
Results
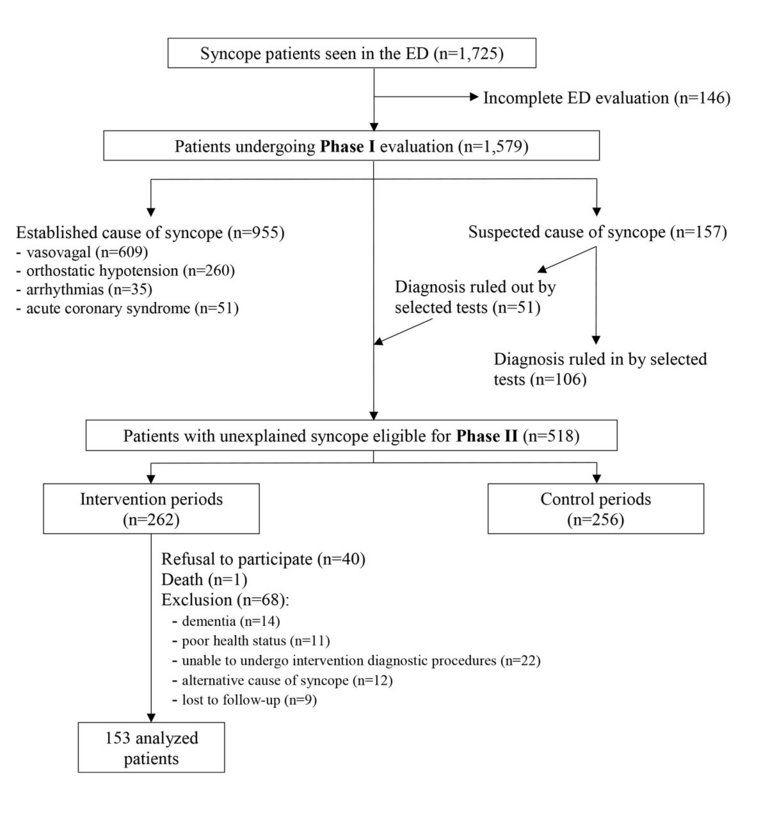
Figure 1 shows the patients flow during the study period. Over the 18-month study period, 1725 (1.2%) of the 144,869 patients seen in the EDs of both hospitals had a chief complaint of syncope. Among these patients, 1579 (92%) entered the phase I evaluation and 146 (8%) were excluded because of an incomplete emergency evaluation. The phase I evaluation permitted a cause for syncope to be established in 67% (n = 1061) of the cases. Thirty three percent (n = 518) of the patients with an unexplained syncope were eligible for the phase II evaluation. Of these, 262 were investigated according to the stepwise diagnostic work-up and followed-up for 1 year. The remaining 256 patients, investigated at the discretion of the ED physicians, were excluded from our study population. Of the 262 patients in the intervention arm, 40 refused to participate, one died from cardiogenic shock, 47 were excluded because of dementia, poor health status or inability to undergo the intervention diagnostic procedures, 12 because of an alternative cause for syncope and 9 because of lost to follow-up at 1 year. The remaining 153 patients included in the intervention period constituted our final study population.
Figure 1
Study design and inclusion scheme. ED = emergency department.
Causes of syncope
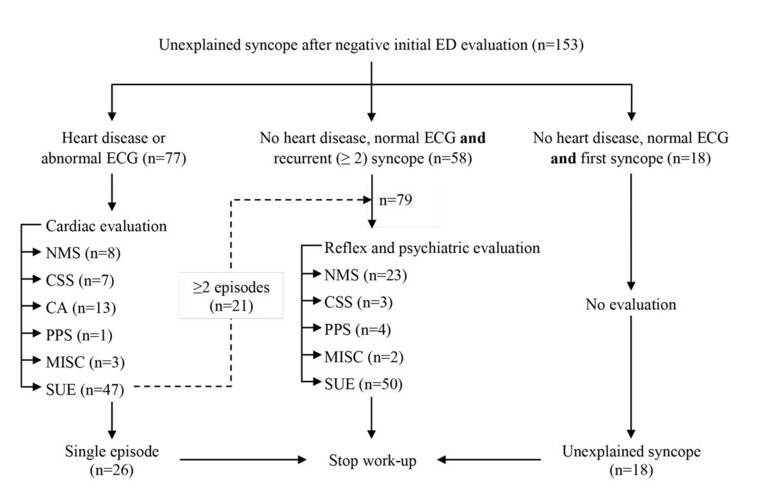
Figure 2 depicts each investigation pathway during the intervention periods. Following the phase II intervention with application of the stepwise diagnostic work-up, a cause for syncope was established in 39% (n = 59) of the 153 patients. Note that five patients had two final diagnoses. NMS was diagnosed in 20% (n = 31) of the cases, cardiac arrhythmias in 8% (n = 13), carotid sinus syndrome in 6% (n = 10), psychogenic pseudo-syncope in 3% (n = 5) and miscellaneous causes in 3% (n = 5). The latter included severe pulmonary hypertension, hypertrophic cardiomyopathy, severe aortic stenosis and postural orthostatic tachycardia syndrome. Sixty one percent (n = 94) of the patients remained with a SUA.
Figure 2
Detailed structured work-up of the intervention protocol in patients with negative initial evaluation (five patients have two diagnosis). CSS = carotid sinus syndrome; CA = cardiac arrhythmias; ED = emergency department; MISC = miscellaneous causes; NMS = neurally mediated syncope; PPS = psychogenic pseudo-syncope; SUA = syncope of unexplained aetiology.
Characteristics of the study population
Table 1 depicts the clinical characteristics of our study population. Patients had a mean age of 62 years with one third over 75 years and 56% were women. An abnormal ECG, including arrhythmias, conduction disorders, Q waves or repolarisation disorders, was present in 42% of the cases. Syncope was a first episode in half of the patients and was preceded by prodromes in two thirds of cases. Syncope led to hospitalisation in 52% and complications in 42% of cases: contusion in 39%, head trauma in 14%, fracture in 5% and car accident in 2%.
Table 1
Clinical characteristics in the different groups of syncope causes..
Total n = 153
SUA n = 94 (61%)
NMS n = 31 (20%)
CA n = 13 (8%)
CSS n = 10 (6%)
MISC n = 5 (3%)
PPS n = 5 (3%)
p-value
Age (y)
62 ± 21
61 ± 20
62 ± 23
75 ± 12
75 ± 15
60 ± 25
39 ± 10
0.006
Age ≥75 years old
55 (36%)
30 (32%)
13 (42%)
7 (54%)
6 (60%)
2 (40%)
0
0.13
Female
86 (56%)
54 (57%)
20 (65%)
3 (23%)
6 (60%)
3 (60%)
3 (60%)
0.22
Number of CRF
1.2 ± 1
1.2 ± 1.1
1.2 ± 0.9
1.6 ± 1.1
1.3 ± 0.9
0.4 ± 0.5
0.6 ± 0.5
0.2
Hypercholesterolaemia
33 (22%)
14 (15%)
8 (26%)
5 (38%)
6 (60%)
0
2 (40%)
0.008
Active smoker
43 (28%)
28 (30%)
10 (32%)
2 (15%)
3 (30%)
0
1 (20%)
0.71
Diabetes mellitus
18 (12%)
13 (14%)
3 (10%)
2 (15%)
1 (10%)
0
0
0.98
Hypertension
70 (46%)
43 (46%)
13 (42%)
10 (77%)
3 (30%)
2 (40%)
0
0.06
Family history of SCD or CAD
16 (11%)
11 (13%)
3 (10%)
2 (15%)
0
0
0
0.92
Past history of CAD
19 (12%)
9 (10%)
4 (13%)
5 (38%)
2 (20%)
1 (20%)
0
0.08
Abnormal ECG
64 (42%)
41 (44%)
7 (23%)
10 (77%)
5 (50%)
3 (60%)
0
0.004
NYHA class >II
9 (6%)
5 (5%)
1 (3%)
0
2 (20%)
1 (20%)
0
0.2
Clinical heart failure
7 (5%)
2 (2%)
2 (6%)
2 (15%)
1 (10%)
1(20%)
0
0.07
Syncope complications
64 (42%)
28 (30%)
19 (61%)
10 (77%)
5 (50%)
3 (60%)
3 (60%)
0.001
Prodromes
102 (67%)
63 (68%)
23 (74%)
7 (54%)
7 (70%)
4 (80%)
3 (60%)
0.83
Symptoms after syncope
82 (54%)
51 (55%)
14 (45%)
8 (62%)
2 (20%)
5 (100%)
4 (80%)
0.04
First episode of syncope
75 (49%)
55 (59%)
7 (23%)
7 (54%)
3 (30%)
2 (40%)
1 (20%)
0.004
Hospitalisation
80 (52%)
42 (45%)
18 (58%)
11 (85%)
7 (70%)
4 (80%)
2 (40%)
0.04
Recurrences
23 (15%)
16 (17%)
4 (13%)
0
1 (10%)
1 (20%)
1 (20%)
0.6
Death
16 (10%)
9 (10%)
3 (10%)
4 (31%)
1 (10%)
0
0
0.34
CA = cardiac arrhythmias; CRF = cardiovascular risk factor; CSS = carotid sinus syndrome; MISC = miscellaneous causes; NMS = neurally mediated syncope; PPS = psychogenic pseudo-syncope; SCD = sudden cardiac death; SUA = syncope of unexplained aetiology. Data are presented as mean ± standard deviation or n (%).
Patients’ characteristics according to syncope causes
Patients’ characteristics in the different groups of syncope causes are shown in Table 1. Patients with cardiac arrhythmias and carotid sinus syndrome causes tended to be older than the other groups, but only the psychogenic pseudo-syncope group was significantly younger (p <0.002). Hypercholesterolaemia was more common in the carotid sinus syndrome group than SUA (p = 0.0032). There was a trend for a higher prevalence of normal ECG in the NMS group than the others, and a significantly higher prevalence of abnormal ECG findings was observed in the cardiac arrhythmia than in the NMS group (p = 0.0016). There were more syncope complications in NMS and cardiac arrhythmia groups than in the SUA group (p <0.003). Past history of syncope was more common in the NMS than in the SUA group (p = 0.0008). The rate of hospitalisation was higher in the cardiac arrhythmia group than in the SUA, but the difference was not significant (p = 0.008).
Comparison of SUA and NMS
Patients with SUA shared most of the clinical and paraclinical characteristics of patients with NMS except for a higher rate of first episode (59 vs 23%, p = 0.001) and a lower rate of syncope complications (30 vs 61%, p = 0.002). Note that the difference in the rate of first episode still remains statistically significant after exclusion of patients with a first syncope episode and a normal ECG who were not further investigated by study design (n = 18, fig. 2).
One-year follow-up
Twenty-three patients (15%) suffered from a syncope recurrence and 16 (10%) died during the 12-month follow-up period. The overall recurrence rate at 12 months was similar (0–20%, p = 0.6) between diagnostic groups, although none of the patients with cardiac arrhythmia syncope had such an event. Importantly, most recurrences occurred in patients with SUA (16 cases, 69% of the total) and the sum of recurrent events in the SUA and NMS groups made up 87% of the total. The death rate was similar between diagnostic groups (0–31%, p = 0.34), although the cardiac arrhythmia group displayed a rather high death rate (31%) during the 12-month follow-up.
Discussion
Our study reports the characteristics, recurrence and mortality rates of patients admitted to the EDs of two university hospitals in whom a standardised work-up established various syncope causes. We hypothesised that patients with a syncope remaining unexplained suffer from some form of NMS.
Comparison of SUA and NMS
The similar clinical and paraclinical characteristics, mortality and recurrence rates between the two groups support our hypothesis. The higher rate of syncope history in the NMS group could be explained by the design of the initial study, as patients with a first episode of syncope, no history of heart disease and a normal ECG where not evaluated for a NMS. Hence, some patients in the SUA group would probably have had a positive tilt-test if it had been performed.
Our hypothesis is also supported by evidence from the literature. The ISSUE and ISSUE-2 [11, 13] studies, which used ILR in patients with syncope and a normal ECG without or with minimal structural heart disease, have shown that the most frequent mechanism during recurrence was prolonged asystole, mainly preceded by progressive bradycardia. This finding is suggestive of a neurally mediated reflex and, importantly, was observed regardless of the tilt-table test result [11, 13]. Solano et al. also showed that a neurally mediated mechanism was the most frequent aetiology for recurrences in patients with SUA without structural heart disease [14].
Susceptibility to vasovagal syncope is difficult to diagnose, in particular with upright tilt testing. Tilt table testing could be negative in cases of typical vasovagal syncope and the sensitivity of this test, even when potentiated with glyceryl trinitrate, was found to be 71% and 75% in patients with typical vasovagal events and situational syncope, respectively [15]. Furthermore, there is a variety of abnormal response to a vasovagal reaction described in the modified VASIS classification [16]. For example, type 3 is characterised by a pure vasodepressor response without bradycardia, hence the use of an ILR could underdiagnose a reflex syncope because of the lack of blood pressure measurements.
In our study, 44 patients in the SUA group (47%) had a tilt-test and the response to the test was classified as normal or not contributory in all the cases. Performing more exhaustive evaluation for susceptibility to reflex mechanisms in all cases of SUA will certainly increase the rate of NMS, but probably have little impact on the management of NMS, except for performing other inappropriate and costly examinations. Indeed, treatment of reflex syncope still lacks standardisation as only a limited number of measures have proved to be of some benefit [17]. Multiple randomised control trials have shown the inability of etilefrine, beta-blockers, fludrocortisone and disopyramide treatment, for instance, to prevent recurrence [18–21]. Two small randomised trials reported a reduced rate of positive tilt test in patients treated with midodrine or a serotonin reuptake inhibitor vs placebo, but data from larger trials are still lacking [22, 23]. More recently, isometric counterpressure manoeuvres and cardiac pacing in severe reflex bradycardia proved to be of some benefit, but in selected patients [17, 24].
Death rate and recurrences
The overall mortality at 1 year of our population was similar to that published in other studies [25]. The death rate was statistically similar between subgroups, although patients with an arrhythmic cause showed a trend towards a higher rate (31%). The latter were older (75 years), had a high number of cardiac risk factors and prevalence of coronary heart disease (38%) and abnormal ECG (77%). The death rate was similar in the SUA and NMS groups. Multiple scores have been developed to predict adverse outcomes in patients with syncope, such as the EGSYS or the OESIL scores [26, 27]. All involved an abnormal ECG and presence of significant structural heart disease such as heart failure or remote myocardial infarction. Our findings are also in line with the Framingham heart study, which showed that the prognosis of NMS is similar to a control population without syncope, and that cardiac syncope had the most adverse outcome [28].
Recurrence rates at 12-month follow-up were rather homogeneous between causes ranging from 10% to 17%, but patients with NMS and SUA accounted for the bulk of recurrences. This is also in line with former studies using ILR in SUA without or with minimal heart disease, where recurrence ranged between 17% and 34% for follow-up of up to 15 months [11, 14, 29]. We found no recurrence in the cardiac arrhythmia group. This may appear paradoxical at first glance, as one would expect patients with cardiac arrhythmias to present a high recurrence rate. The treatment of syncopal arrhythmias is rather straightforward as it directly targets the underlying mechanism such as rate or rhythm control for atrial fibrillation, implantation of devices for bradycardia or ventricular tachyarrhythmias. In our study, 13% of the NMS patients presented a recurrence at 12 months. These patients could have been the right candidates for cardiac pacing if severe bradycardia had been established with an ILR as shown in the ISSUE 3 trial [17]. These data, however, were not available at the time of our study. Finally, the similar death and recurrence rates of patients with SUA and NMS fit with their similar clinical characteristics, reinforcing the evidence that SUA patients mostly suffered from some form of NMS.
Limitations
First, ILR, which would have reinforced the accuracy of established causes of syncope, was not part of our study design. Second, ECGs with leads V1 and V2 at the second or third intercostal space and an ajmaline test were not systematically performed; hence some cases of transient type 1 Brugada syndrome might have been underdiagnosed. Third, because of the small sample size, our study may be underpowered to show differences between groups, in particular between the SUA and NMS patients. Forth, the high rate of exclusion could represent a bias as most excluded patients were old with cognitive dysfunction, which, as shown in the literature, is commonly associated with hypotensive disorders [30]. By study design, patients from the initial screening who were excluded because of refusal, dementia or poor health status were not kept in a separate database. We were, however, able to compare the clinical characteristics of the 21 patients excluded because of lack of follow-up or because of an alternative cause with those of the included population. There was no significant difference. Finally, the follow-up was limited to 1 year and only established whether our patients suffered from a recurrence or were alive, but was not designed to establish causes of death or syncope recurrence.
Financial disclosure
This study was funded by the Swiss National Science Foundation (32-64940.01).
Correspondence
Laurent Froidevaux, HFR hôpital de Riaz, Rue de l’hôpital 9, Case postale 70, CH-1632 Riaz, laurent.froidevaux[at]h-fr.ch
References
1Brignole M, Moya A, de Lange FJ, Deharo J-C, Elliott PM, Fanciulli A, et al.; ESC Scientific Document Group. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39(21):1883–948. doi:. http://dx.doi.org/10.1093/eurheartj/ehy037PubMed
2Day SC, Cook EF, Funkenstein H, Goldman L. Evaluation and outcome of emergency room patients with transient loss of consciousness. Am J Med. 1982;73(1):15–23. doi:. http://dx.doi.org/10.1016/0002-9343(82)90913-5PubMed
4Brignole M, Menozzi C, Bartoletti A, Giada F, Lagi A, Ungar A, et al.A new management of syncope: prospective systematic guideline-based evaluation of patients referred urgently to general hospitals. Eur Heart J. 2006;27(1):76–82. doi:. http://dx.doi.org/10.1093/eurheartj/ehi647PubMed
5Sarasin FP, Louis-Simonet M, Carballo D, Slama S, Rajeswaran A, Metzger JT, et al.Prospective evaluation of patients with syncope: a population-based study. Am J Med. 2001;111(3):177–84. doi:. http://dx.doi.org/10.1016/S0002-9343(01)00797-5PubMed
6Ammirati F, Colivicchi F, Santini M. Diagnosing syncope in clinical practice. Implementation of a simplified diagnostic algorithm in a multicentre prospective trial - the OESIL 2 study (Osservatorio Epidemiologico della Sincope nel Lazio). Eur Heart J. 2000;21(11):935–40. doi:. http://dx.doi.org/10.1053/euhj.1999.1910PubMed
7Croci F, Brignole M, Alboni P, Menozzi C, Raviele A, Del Rosso A, et al.The application of a standardized strategy of evaluation in patients with syncope referred to three syncope units. Europace. 2002;4(4):351–5. doi:. http://dx.doi.org/10.1053/eupc.2002.0267PubMed
8Blanc J-J, L’Her C, Touiza A, Garo B, L’Her E, Mansourati J. Prospective evaluation and outcome of patients admitted for syncope over a 1 year period. Eur Heart J. 2002;23(10):815–20. doi:. http://dx.doi.org/10.1053/euhj.2001.2975PubMed
9Farwell DJ, Sulke AN. Does the use of a syncope diagnostic protocol improve the investigation and management of syncope?Heart. 2004;90(1):52–8. doi:. http://dx.doi.org/10.1136/heart.90.1.52PubMed
10Moya A, Sutton R, Ammirati F, Blanc JJ, Brignole M, Dahm JB, et al.; Task Force for the Diagnosis and Management of Syncope; European Society of Cardiology (ESC); European Heart Rhythm Association (EHRA); Heart Failure Association (HFA); Heart Rhythm Society (HRS). Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J. 2009;30(21):2631–71. doi:. http://dx.doi.org/10.1093/eurheartj/ehp298PubMed
11Moya A, Brignole M, Menozzi C, Garcia-Civera R, Tognarini S, Mont L, et al.; International Study on Syncope of Uncertain Etiology (ISSUE) Investigators. Mechanism of syncope in patients with isolated syncope and in patients with tilt-positive syncope. Circulation. 2001;104(11):1261–7. doi:. http://dx.doi.org/10.1161/hc3601.095708PubMed
12Sarasin FP, Pruvot E, Louis-Simonet M, Hügli OW, Sztajzel JM, Schläpfer J, et al.Stepwise evaluation of syncope: a prospective population-based controlled study. Int J Cardiol. 2008;127(1):103–11. doi:. http://dx.doi.org/10.1016/j.ijcard.2007.04.077PubMed
13Brignole M, Sutton R, Menozzi C, Garcia-Civera R, Moya A, Wieling W, et al.; International Study on Syncope of Uncertain Etiology 2 (ISSUE 2) Group. Early application of an implantable loop recorder allows effective specific therapy in patients with recurrent suspected neurally mediated syncope. Eur Heart J. 2006;27(9):1085–92. doi:. http://dx.doi.org/10.1093/eurheartj/ehi842PubMed
14Solano A, Menozzi C, Maggi R, Donateo P, Bottoni N, Lolli G, et al.Incidence, diagnostic yield and safety of the implantable loop-recorder to detect the mechanism of syncope in patients with and without structural heart disease. Eur Heart J. 2004;25(13):1116–9. doi:. http://dx.doi.org/10.1016/j.ehj.2004.05.013PubMed
15Furukawa T, Maggi R, Solano A, Croci F, Brignole M. Effect of clinical triggers on positive responses to tilt-table testing potentiated with nitroglycerin or clomipramine. Am J Cardiol. 2011;107(11):1693–7. doi:. http://dx.doi.org/10.1016/j.amjcard.2011.01.057PubMed
16Brignole M, Menozzi C, Del Rosso A, Costa S, Gaggioli G, Bottoni N, et al.New classification of haemodynamics of vasovagal syncope: beyond the VASIS classification. Analysis of the pre-syncopal phase of the tilt test without and with nitroglycerin challenge. Vasovagal Syncope International Study. Europace. 2000;2(1):66–76. doi:. http://dx.doi.org/10.1053/eupc.1999.0064PubMed
17Brignole M, Menozzi C, Moya A, Andresen D, Blanc JJ, Krahn AD, et al.; International Study on Syncope of Uncertain Etiology 3 (ISSUE-3) Investigators. Pacemaker therapy in patients with neurally mediated syncope and documented asystole: Third International Study on Syncope of Uncertain Etiology (ISSUE-3): a randomized trial. Circulation. 2012;125(21):2566–71. doi:. http://dx.doi.org/10.1161/CIRCULATIONAHA.111.082313PubMed
18Raviele A, Brignole M, Sutton R, Alboni P, Giani P, Menozzi C, et al.Effect of etilefrine in preventing syncopal recurrence in patients with vasovagal syncope: a double-blind, randomized, placebo-controlled trial. The Vasovagal Syncope International Study. Circulation. 1999;99(11):1452–7. doi:. http://dx.doi.org/10.1161/01.CIR.99.11.1452PubMed
19Madrid AH, Ortega J, Rebollo JG, Manzano JG, Segovia JG, Sánchez A, et al.Lack of efficacy of atenolol for the prevention of neurally mediated syncope in a highly symptomatic population: a prospective, double-blind, randomized and placebo-controlled study. J Am Coll Cardiol. 2001;37(2):554–9. doi:. http://dx.doi.org/10.1016/S0735-1097(00)01155-4PubMed
20Morillo CA, Leitch JW, Yee R, Klein GJ. A placebo-controlled trial of intravenous and oral disopyramide for prevention of neurally mediated syncope induced by head-up tilt. J Am Coll Cardiol. 1993;22(7):1843–8. doi:. http://dx.doi.org/10.1016/0735-1097(93)90767-UPubMed
21Sheldon R, Raj SR, Rose MS, Morillo CA, Krahn AD, Medina E, et al.; POST 2 Investigators. Fludrocortisone for the Prevention of Vasovagal Syncope: A Randomized, Placebo-Controlled Trial. J Am Coll Cardiol. 2016;68(1):1–9. doi:. http://dx.doi.org/10.1016/j.jacc.2016.04.030PubMed
22Romme JJCM, van Dijk N, Go-Schön IK, Reitsma JB, Wieling W. Effectiveness of midodrine treatment in patients with recurrent vasovagal syncope not responding to non-pharmacological treatment (STAND-trial). Europace. 2011;13(11):1639–47. doi:. http://dx.doi.org/10.1093/europace/eur200PubMed
23Theodorakis GN, Leftheriotis D, Livanis EG, Flevari P, Karabela G, Aggelopoulou N, et al.Fluoxetine vs. propranolol in the treatment of vasovagal syncope: a prospective, randomized, placebo-controlled study. Europace. 2006;8(3):193–8. doi:. http://dx.doi.org/10.1093/europace/euj041PubMed
24Baron-Esquivias G, Morillo CA, Moya-Mitjans A, Martinez-Alday J, Ruiz-Granell R, Lacunza-Ruiz J, et al.Dual-Chamber Pacing With Closed Loop Stimulation in Recurrent Reflex Vasovagal Syncope: The SPAIN Study. J Am Coll Cardiol. 2017;70(14):1720–8. doi:. http://dx.doi.org/10.1016/j.jacc.2017.08.026PubMed
25Solbiati M, Casazza G, Dipaola F, Rusconi AM, Cernuschi G, Barbic F, et al.Syncope recurrence and mortality: a systematic review. Europace. 2015;17(2):300–8. doi:. http://dx.doi.org/10.1093/europace/euu327PubMed
26Del Rosso A, Ungar A, Maggi R, Giada F, Petix NR, De Santo T, et al.Clinical predictors of cardiac syncope at initial evaluation in patients referred urgently to a general hospital: the EGSYS score. Heart. 2008;94(12):1620–6. doi:. http://dx.doi.org/10.1136/hrt.2008.143123PubMed
27Colivicchi F, Ammirati F, Melina D, Guido V, Imperoli G, Santini M; OESIL (Osservatorio Epidemiologico sulla Sincope nel Lazio) Study Investigators. Development and prospective validation of a risk stratification system for patients with syncope in the emergency department: the OESIL risk score. Eur Heart J. 2003;24(9):811–9. doi:. http://dx.doi.org/10.1016/S0195-668X(02)00827-8PubMed
28Soteriades ES, Evans JC, Larson MG, Chen MH, Chen L, Benjamin EJ, et al.Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878–85. doi:. http://dx.doi.org/10.1056/NEJMoa012407PubMed
29Menozzi C, Brignole M, Garcia-Civera R, Moya A, Botto G, Tercedor L, et al.; International Study on Syncope of Uncertain Etiology (ISSUE) Investigators. Mechanism of syncope in patients with heart disease and negative electrophysiologic test. Circulation. 2002;105(23):2741–5. doi:. http://dx.doi.org/10.1161/01.CIR.0000018125.31973.87PubMed
30Testa G, Ceccofiglio A, Mussi C, Bellelli G, Nicosia F, Bo M, et al.Hypotensive Drugs and Syncope Due to Orthostatic Hypotension in Older Adults with Dementia (Syncope and Dementia Study). J Am Geriatr Soc. 2018;66(8):1532–7. doi:. http://dx.doi.org/10.1111/jgs.15421PubMed