Aggressive surgical management of patients with severe aortic stenosis and concomitant Fabry disease should be the treatment of choice, even during enzyme replacement therapy.
Introduction
Fabry disease is an X-linked glycosphingolipid disorder, homozygous in men and heterozygous in women, caused by deficient activity of enzyme α-galactosidase, which results in the systemic accumulation of globotriosylceramide (Gb3) in all tissues of the body, such as skin, kidney, cornea and the heart. Globotriaosylceramide can be stored in various cells of the heart, such as cardiomyocytes, conduction system cells, valvular fibroblasts, endothelial cells within all types of vessels and vascular smooth muscle cells [1, 2]. This storage can cause progressive hypertrophy of the cardiac muscles, with increasing interstitial and fibrotic changes. As a result, there is severe left ventricular hypertrophy, ischaemia and cardiac events, impaired left ventricular function, arrhythmias and valvular involvement. The treatment of choice in Fabry disease is enzyme replacement, with remarkable improvement of the cardiac symptoms [1, 2].
Case report
A 50-year-old male with Fabry disease, treated with recombinant α-galactosidase enzyme replacement therapy (0.2 mg/kg per infusion) for 14 years, and severe aortic stenosis was admitted for aortic valve replacement.
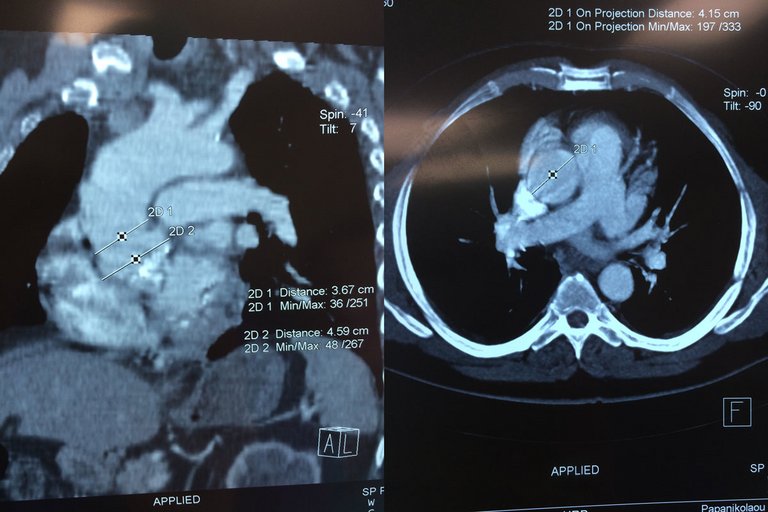
The clinical background included New York Heart Association (NYHA) class II status, chronic obstructive pulmonary disease, systemic hypertension and dyslipidaemia. His kidney function was normal, with serum creatinine 0.6 mg/dl. Standard 12-lead electrocardiography revealed left ventricular hypertrophy and a prolonged P-R interval. Thoracic echocardiography showed severe concentric left ventricular hypertrophy (posterior wall thickness in end-diastole 13.3 mm) with an ejection fraction of 74%, left ventricular diastolic dysfunction, severe aortic valve stenosis with peak gradient 120 mmHg, associated mild aortic regurgitation, moderate mitral valve stenosis (mitral valve area 1.5 cm2) and moderate dilation of the Valsalva sinus at about 43 mm (fig. 1). His spirometry results where within normal limits. A Holter report indicated normal sinus rhythm with minimum ventricular systoles and ectopic atrial systoles. There was no significant coronary artery disease on coronary angiography. Preoperative computed tomography angiography showed moderate dilation of the Valsalva sinus at about 46 mm and the ascending aorta was 41 mm in diameter (fig. 2).
Figure 1
Heart U/S showing severe aortic valve stenosis with peak gradient estimated at 120mmHg.
Figure 2
Chest CT showing aortic valve dilation.
The patient was a young male without indications for transcatheter aortic valve implantation (TAVI) (as defined by risk scores and other comorbidities) [3, 4], so he underwent a median sternotomy and aortic valve replacement with mechanical valve No 23, with right atrium and left ventricular wall biopsies under cardiopulmonary bypass. Cold blood cardioplegia was used to protect the myocardium intraoperatively. After careful examination of the aorta during surgery, a decision was made not to replace it. Postoperatively, the patient had sinus rhythm with ectopic ventricular systoles. His serum creatinine was increased to 2.3 mg/dl on postoperative day 1, with a gradual decrease during the following days.
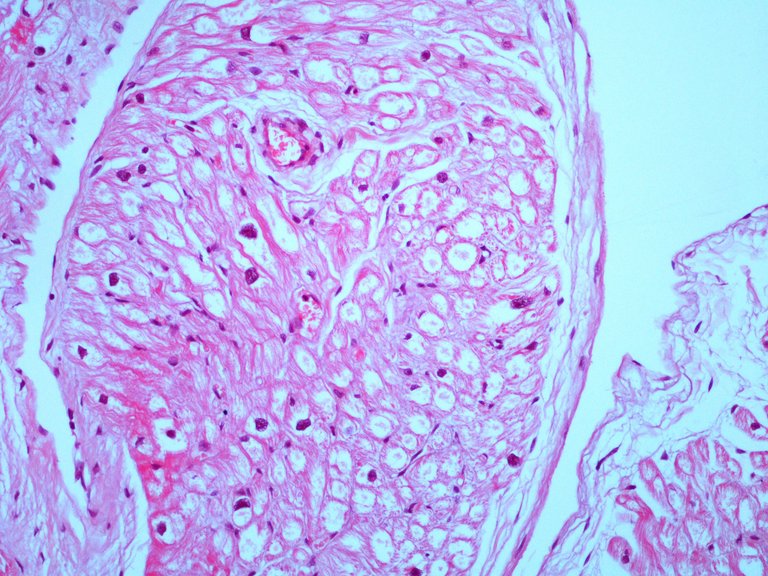
Histological examination of the aortic valve showed loss of the valve architecture with excessive degeneration including oedema, myxoid degeneration and calcification. Cardiac biopsies from the left ventricular wall and the right atrium revealed groups of muscle fibres with size and diameter within normal limits. Some fibres appeared slightly hypertrophic with large nuclei. Myocite vacuoles were also reported (fig. 3). No sign of inflammation or necrosis was observed. Postoperative cardiac ultrasound showed good function of the mechanical aortic valve and a normal left ventricular ejection fraction, with a moderate mitral valve stenosis similar to that in the preoperative ultrasound.
The patient was discharged on the fifth postoperative day. Follow-up ultrasound 1 month later showed similar findings to the one on discharge day, with good valve function and moderate mitral valve stenosis.
Discussion
Fabry disease is a rare disorder with X-chromosomal inheritance. The disease is induced by mutation in the α-galactosidase A gene (GLA), causing a deficiency of the hydrolase α-galactosidase A (α-GalA). As a result, the inability for glabotriaosylceramide (Gb3) to be metabolised leads to progressive intracellular storage of the Gb3 in various tissues and organs and elevated plasma levels of lyso-Gb3. Heart, the vascular endothelium of the kidney, nervous system, eyes and skin are the most commonly affected organs. Because of to its clinical symptoms and frequent lesions on magnetic resonance imaging, Fabry disease is commonly misdiagnosed as multiple sclerosis. It is clear that its clinical manifestations are very diverse and its differential diagnosis is correspondingly broad. Thus there is often a delay before the diagnosis of Fabry disease is established, with a time period from symptom onset to the correct diagnosis of 13 years in men and 17 years in women [5].
Cardiac involvement includes hypertrophy, arrhythmias, ischaemia, impaired left ventricular function and valvular disorders [1, 2, 6, 7]. In 2000, Linhart et al. identified mitral and aortic abnormalities in 17 (57%) and 14 (47%), respectively, of 30 patients with Fabry disease [8]. Kampmann et al. indicated that there was mild insufficiency in the aortic and mitral valve in 14 (25.5%) and 14 (25.5%) patients, respectively. They also reported a mitral prolapse in 6 (10.9%) of 50 patients with Fabry disease [9]. In another paper from Iwase et al., a 46-year-old male with Fabry disease and with aortic regurgitation and complete atrioventricular block did not undergo surgical treatment [10]. However, Choi et al reported a case of a 31-year-old male with Fabry disease and aortic regurgitation who did undergo valvular replacement during enzyme replacement therapy [11]. Giustino et al were the first to report a case of a 76-year-old patient with Fabry disease and low gradient aortic valve stenosis, who underwent TAVI [12].
In the current TAVI era, even though surgical aortic valve replacement (SAVR) remains the golden standard for severe aortic stenosis, patients with associated high surgical risk status (as defined by risk scores and other comorbidities) should be recommended TAVI. Moreover, in a substudy of the PARTNER trial in patients with LV dysfunction and high surgical risk, mortality rates and LV functional recovery were comparable between TAVI and SAVR [12]. However, our patient did not match the TAVI criteria (no impaired left ventricular function, no kidney failure, etc.). Most importantly, there was no extension of the disease to other organs, possibly because he was under enzyme replacement therapy at the time of operation.
Histology of the aortic valve showed loss of the valve architecture with excessive degeneration, including oedema, myxoid degeneration and calcification. Such findings are similar to those of other patients with severe aortic stenosis who were treated surgically. However, cardiac biopsies showed groups of muscle fibres with size and diameter within normal limits. Some fibres appeared slightly hypertrophic with large nuclei and myocite vacuoles, a hallmark of Fabry disease. Valvular involvement in patients with Fabry disease can occur as a result of infiltrative changes within the valvular fibres. This leads to valvular thickening and deformation.
Patients with Fabry disease and mitral valve prolapse, mild to moderate valvular regurgitation and aortic root dilation rarely require surgical intervention, according to literature. Nonetheless, severe aortic stenosis is an extremely rare disorder and in its management surgery is of the essence.
To our knowledge this is the first case report in literature of a patient with Fabry disease and severe aortic stenosis who underwent surgical valvular replacement with a mechanical valve during enzyme replacement therapy, with consideration of the affected myocardium and the according operative risk. Aggressive surgical treatment should be encouraged in such cases. Clinical outcomes for patients with Fabry disease and severe aortic stenosis who undergo surgery are quite beneficial, as our case report indicates.
Conclusion
Surgical management of patients with severe aortic stenosis and concomitant Fabry disease should be the treatment of choice, even during enzyme replacement therapy.
Correspondence
Athanasia Vlahou, PhD, “George Papanikolaou” General Hospital, GR-57010 Exohi,Thessaloniki, Vlahouathanasia[at]gmail.com
2Linhart A. The heart in Fabry disease. In: Mehta A, Beck M, Sunder-Plassmann G, editors. Fabry Disease: Perspectives from 5 Years of FOS. Oxford: Oxford PharmaGenesis; 2006. Chapter 20
3Mylotte D, Martucci G, Piazza N. Patient selection for transcatheter aortic valve implantation: An interventional cardiology perspective. Ann Cardiothorac Surg. 2012;1(2):206–15. PubMed
4Kappetein AP, Head SJ, Généreux P, Piazza N, van Mieghem NM, Blackstone EHUpdated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. Eur Heart J. 2012;33(19):2403–18. doi:. http://dx.doi.org/10.1093/eurheartj/ehs255PubMed
7Oikawa M, Sakamoto N, Kobayashi A, Suzuki S, Yoshihisa A, Yamaki TFamilial hypertrophic obstructive cardiomyopathy with the GLA E66Q mutation and zebra body. BMC Cardiovasc Disord. 2016;16(1):83. doi:. http://dx.doi.org/10.1186/s12872-016-0262-yPubMed
8Linhart A, Palecek T, Bultas J, Ferguson JJ, Hrudová J, Karetová DNew insights in cardiac structural changes in patients with Fabry’s disease. Am Heart J. 2000;139(6):1101–8. doi:. http://dx.doi.org/10.1067/mhj.2000.105105PubMed
9Kampmann C, Baehner F, Whybra C, Martin C, Wiethoff CM, Ries MCardiac manifestations of Anderson-Fabry disease in heterozygous females. J Am Coll Cardiol. 2002;40(9):1668–74. doi:. http://dx.doi.org/10.1016/S0735-1097(02)02380-XPubMed
10Iwase M, Yamauchi K, Maeda M, Aoki T, Yokota M, Hayashi H[Echocardiographic findings in a case of Fabry’s disease with aortic regurgitation and complete AV block, and in his family members]. J Cardiol. 1988;18(2):589–98. Article in Japanese. PubMed
12Giustino G, Chieffo A, Montorfano M, Spagnolo P, Panoulas VF, Bernelli CFirst case reported of transcatheter aortic valve implantation in a patient affected by Fabry s Disease and severe low-flow low-gradient aortic valve stenosis. Case Rep Intern Med. 2014;1(2):71–4. doi:. http://dx.doi.org/10.5430/crim.v1n2p71