Joint Annual Meeting 2019 of the Swiss Society of Cardiology and the Swiss Society of Cardiac Surgery
P92
MiECC - proof of a novel concept for a minimal invasive extracorporeal perfusion system in pediatric congenital cardiac surgery
P.P. Heinisch1, M. Bartkevics1, S. Wyss1, H.-J. Jenni1, H. Widenka1, G. Erdoes2, B. Eberle2, T. Carrel1, A. Kadner1
1Center for Congenital Heart Disease, Department of Cardiovascular Surgery, 2Department of Anaesthesiology and Pain Medicine, Inselspital Bern, Berne, Switzerland
Introduction: Minimal invasive extracorporeal circulation (MiECC) circuits are an alternative to conventional extracorporeal circulation (CECC). Based on the positive effects and improved perioperative outcomes of MiECC in adult cardiac surgery, this perfusion concept appears particularly attractive to pediatric cardiac surgery. So far, there are no reports on the clinical application of a MiECC for corrective surgery in neonates and children. We report our initial experiences by using a MiECC system in paediatric cardiac surgery.
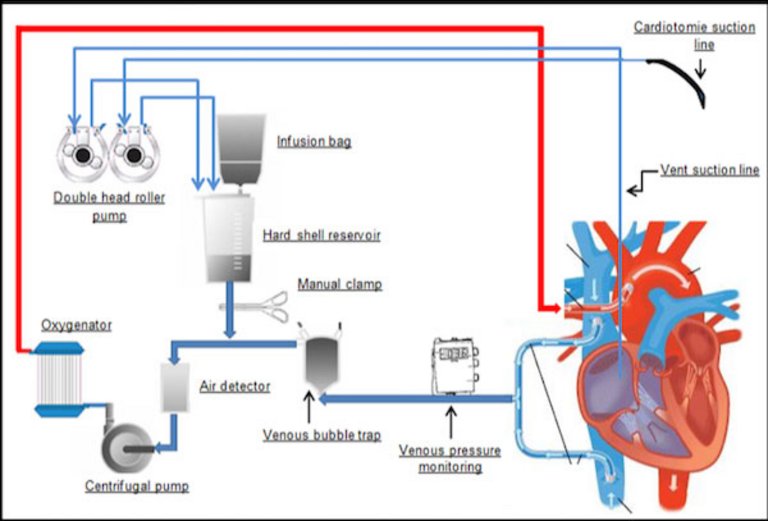
Methods: A total of 38 pediatric patients underwent surgical interventions for a variety of congenital heart disease from March 2017 until August 2018 with a MiECC. Following the classification of MiECC circuits by the Minimal invasive Extra-Corporeal Technologies International Society(MiECTIS), Type I and Type III closed perfusion circuits were assembled depending on the planned intervention: Type I for closed heart interventions and Type III for open heart procedures (Figure P92-1). Primary outcome was conversion to CECC, secondary endpoints included major adverse cardiac or cerebrovascular events (MACCE).
Results: MiECC perfusion was successfully performed in all patients (100%). Median patient age was 9.5 months (range 0.2 - 176) with a median weight of 8.1 kg (range 2.3 - 49). For both MiECC types no system related technical complications were encountered. Beating heart procedures were performed in 23 cases (60%) at normothermia, while in 15 (40%) interventions cardioplegic cardiac arrest was induced at mild hypothermia. All patients had an uneventful perioperative course with no in-hospital mortality. MACCE did not occur during the hospitalization period.
Conclusions: MiECC can be performed by using standard techniques for closed and open cardiac procedures for the correction of a variety of malformations in neonates and children with good results and uneventful postoperative course.
Figure
P92-1. Schematic overview for a modular MiECC type III circuit with additional components.
P93
VRAMT - a less invasive and cosmetically more attractive alternative to median sternotomy for the correction of a variety of congenital heart defects
P.P. Heinisch1, M.J. Beck1, M. Wildbolz2, B. Eberle3, D. Hutter2, G. Erdoes3, J.-P. Pfammatter2, M. Glöckler2, T. Humpl4, T. Carrel1, A. Kadner1
1Centre for Congenital Heart Disease, Department of Cardiovascular Surgery, 2Centre for Congenital Heart Disease, Department of Cardiology, 3Department of Anaesthesiology and Pain Therapy, 4Pediatric Intensive Care Unit, Inselspital Bern, Berne, Switzerland
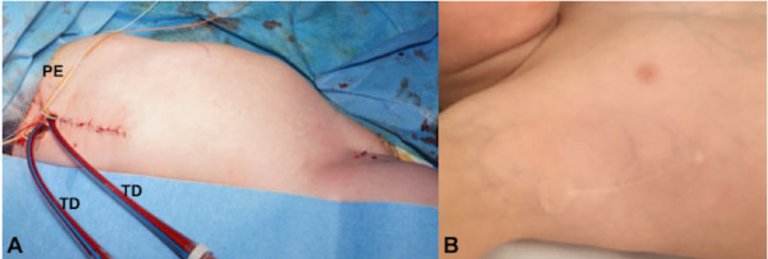
Introduction: Vertical right axillary mini-thoracotomy (VRAMT) represents a less invasive and cosmetically attractive alternative to the standard approach for the correction of congenital heart defects the median sternotomy. Here we present our institutional experience with VRAMT and its expansion to the correction of more complex heart defects.
Methods: Retrospective analysis of patients up to 16 years of agewho underwent corrective cardiac surgery by VRAMT starting from January 2012 until October 2018 were included. The peri, intra-, and postoperative data of all patients undergoing surgical correction for congenital heart defects through VRAMT were retrospectively analyzed. The surgical technique for VRAMT involved a 4-5 cm vertical skin incision in the right axilla and central aortic cannulation. The study was approved by the ethics committee (Approval Nr. 2016-01484) of the canton of Bern, Switzerland.
Results: In total 110 patients were included in this study with the following cardiac diagnoses: Atrial septal defects secundum type (35), ventricular septal defects (44), complete atrioventricular septal defects (12), partial atrioventricular septal defects (7),partial anomalous pulmonary venous connection(9), double chambered right ventricle (1), and Cor triatriatum (2). The mean age of patients was 3.56 (±3.73) years, mean body weight was 13.18 (±9.09) kg. Mean Cardio-pulmonary bypass time was at 70.52 (±28.74) minutes, mean cross-clamping time of the aorta was 42.52 (±15.73) minutes. Mean intensive care stay was 84.03 (±68.54) hours, while overall hospital stay resulted in a mean of 8.36 (±4.37) days. There was no early or late mortality. There was no need for any conversion from VRAMT to median sternotomy in any case. No wound infection nor thoracic deformities were observed (Figure P93-1). The mean clinical and echocardiographic follow up time was 11.57 (±14.90) months.
Conclusions: VRAMT can be considered as a safe and feasible access for the repair of a wide range of congenital heart defects. This minimally invasive technique has become the standard approach for the correction of congenital heart defects at our institution. For selected patient groups, it can also be expanded to more complex heart defects such as complete atrioventricular septal defects without compromising the surgical result and clinical outcome.
P94
Early experience with a novel, absorbable, knotless suture device for sternal closure and healing in pediatric cardiac surgery
P.P. Heinisch1, M. Bartkevics1, H. Widenka1, G. Erdoes2, D. Hutter3, M. Glöckler3, T. Carrel1, A. Kadner1
1Centre for Congenital Heart Disease, Department of Cardiovascular Surgery, 2Department of Anaesthesiology and Pain Therapy, 3Centre for Congenital Heart Disease, Department of Cardiology, Inselspital Bern, Berne, Switzerland
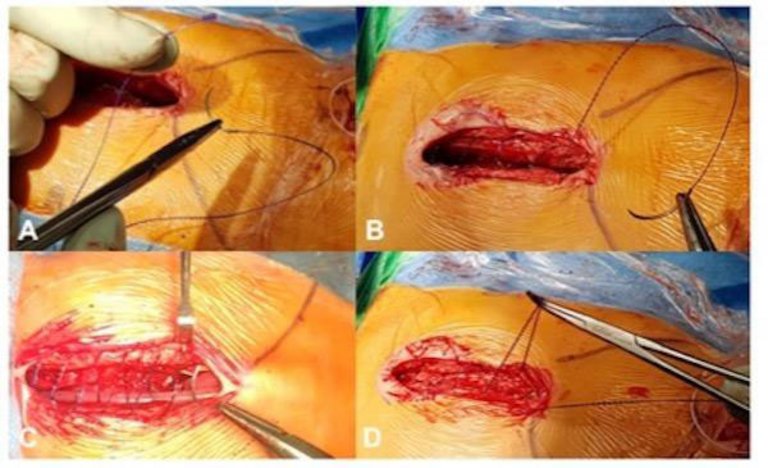
Introduction: Sternal closure by absorbable suture material is an established method for chest closure in pediatric cardiac surgery. However, the formation of granuloma around knotted suture material is frequently observed and has potential for prolonged wound healing and infection, particularly in newborns and infants. This study analyses the suitability and reliability of a novel absorbable, self-locking multi-anchor knotless suture with antibacterial technology for sternal closure in pediatric cardiac surgery.
Methods: The applied material (STRATAFIX™ Symmetric PDS Plus, Ethicon) presents a poly-dioxanon PDS suture with a self-locking multi anchor design which enables a sternal closure in a continuous knotless suture technique (Figure P94-1). The duration until complete absorption is reported of approximately 120-180 days. All children undergoing knot-less closure after standard median sternotomy were examined for the occurrence of any sternal wound infection or instability by applying the screening criteria of the Centres for Disease Control and Prevention (CDC) at discharge, 30 and 60 days.
Results: In 130 cases, the new knot-less sternal closure was used. Mean age was 19.0 ±31.9 months (range: 0.03 to 142 months), mean bodyweight 7.8 ±6.5 kg (range: 2.4 to 35 kg). The main cardiac pathologies were tetralogy of Fallot (n = 27, 20.8%), transposition of the great arteries (n = 21, 16.2%), hypoplastic-left-heart-syndrome (n = 15, 11.5%), pulmonary stenosis (n = 8, 6.2%), pulmonary atresia (n = 7, 5.4%) and other cardiac diagnoses. Open-thorax treatment with delayed sternal closure occurred in 22 cases with a mean closure after 1.95±1.2 days. No cases of deep sternal site infection or instability were observed.
Conclusions: The application of the absorbable, knot-less suture technique provides excellent results regarding the rate of sternal wound infection and improved healing after median sternotomy in pediatric patients.
Figure
P94-1.
P95
Cardiac remodeling in children with infantile pompe disease under enzyme replacement therapy, a single center retrospective analysis
A. Oxenius1, M. Rohrbach2, R. Weber1, C. Balmer1, E. Valsangiacomo Büchel1, A. Cavigelli-Brunner1
1Kinderherzzentrum Zürich, 2Metabolic Disease, Children Hospital, University of Zurich, Zurich, Switzerland
Introduction: Infantile Pompe (IP) disease is an inheritable metabolic disorder caused by deficiency of acid α-glucosidase (GAA) resulting in glycogen accumulation in the lysosomes of many tissues. Within the heart it is characterized by progressive hypertrophic cardiomyopathy in early infancy. Heart failure is one of the main causes of death in the first year of life. The introduction of enzyme replacement therapy (ERT) can reduce or even reverse hypertrophy and improves cardiac function leading to increased survival. We describe our experience of cardiac remodelling under ERT.
Methods: Retrospective observational single center study from 2006 - 2018.
Results: 5 children (3 males) were included in the study. All but one were CRIM (cross-reactive immunologic material) positive. Median age at diagnosis was 4 months (0-15); in one patient IP was known prenatally. ERT was started immediate after diagnosis at a mean weight of 5.8 ± 2.4kg. At start of the ERT all infants had a concentric hypertrophy with preserved cardiac function. Septum thickness was ranging from 6-16mm, indexed cardiac mass was median 272 g/m2 (72-332). One patient died after 3 months of ERT due to severe respiratory failure. In the four others cardiac mass normalized under ERT after a median duration of 6 months (1-10). One child had allergic reaction type II on ERT but could continue the therapy on monoclonal anti-immunglobulin E antibody. Median Follow up was 19 months (8-144). On resting electrocardiogram the PR-interval was shortened in all patients with a median duration of 80ms (60-114) and increased to normal by study end in 2 patients. Supraventricular tachycardias were observed in two patients, one with preexcitation who underwent successful radiofrequency ablation of a left posterior pathway at the age of 8 years. The former receives antiarrhythmic drug therapy until study end.
Conclusions: ERT significantly reduces cardiac hypertrophy in infantile Pompe disease and improves survival. The typically short PR interval however may remain and arrhythmias may persist even throughout longer follow up period.
P96
One stage correction of long tracheal stenosis and congenital heart disease
R. Pfister1, T. Sologashvili2, P. Myers1, N. Sekarski1, M. Beghetti2, R. Pretre1
1CHUV, Lausanne, 2HUG, Geneva, Switzerland
Introduction: The association of congenital heart defects (CHD) and long segment tracheal stenosis (CTS) is rare and is a high-risk situation for newborns and infants. Concomitant treatment remains challenging. We review our surgical results of concomitant surgical correction under extracorporeal circulation (ECC).
Method: From March 1999 to January 2019, 15 patients, (9 male and 7 female; mean age 27 months, mean weight 10 kg at the time of operation) with associated CTS and CHD were operated on ECC. 8 patients had the CTS diagnosis only during the cardiac preoperative evaluation. Clinical features in the other patients were stridor in 2, respiratory infection in 3 and both in 3 patients. Minimal tracheal rings were 3 and the maximum was all trachea. Among these patients, 7 had a tracheal bronchus. A slide tracheoplasty was performed in all patients concomitant to the CHD surgery in 14 patients. 1 patient was operated in emergency of a truncus arteriosus and the tracheoplasty could be performed only after 2 weeks. CHD surgery consisted of 3 tetralogies of Fallot, 2 pulmonary atresias with ventricular septal defect type A, 4 ventricular septal defects, 4 left pulmonary artery (LPA) slings, and 1 partial anomalous pulmonary venous return.
Result: There were no early or late deaths. Median ECC times was 189 min (range from 145 to 425 min). There was no clamping in sling patients. Median clamping time was 55 min in the others (range from 20 to 104 min). 1 patient required extracorporeal membrane oxygenation 48 hours after the procedure for respiratory acidosis. 1 patient required reopening of the sternum for a RV dysfunction. There was no need for delayed sternal closure in the remaining patients. Concerning the pulmonary slings, 1 had a postoperative thrombus with favorable evolution under anticoagulation and 1 needed reoperation for a kinking of the LPA. Concerning the tracheal repair, 5 patients presented some anastomotic granulations which needed endobronchial treatment and 5 patients (3 with granulation) required temporary stenting of the airways. Median time to extubation was 6.5 days.
Conclusion: Slide tracheoplasty is a good option in case of concomitant congenital heart disease even if it can required prolonged extracorporeal circulation. Complete extensive treatment of both pathologies was achievable with satisfactory results.
P97
4D vs. 2D phase-contrast cardiac magnetic resonance for blood flow quantification in congenital heart disease
M. Prsa1, E. Tenisch2, D. Piccini2, N. Jin3, J. Bouchardy4, C. Blanche5, N. Sekarski1, A.G. Pavon6, G. Vincenti6, D. Rodrigues2, M. Stuber2, J. Schwitter7, T. Rutz7
1Paediatric Cardiology Unit, 2Department of Radiology, University Hospital of Lausanne and University of Lausanne, Lausanne, Switzerland, 3Cardiovascular MR R&D, Siemens Medical Solutions, Cleveland, OH, United States, 4Service of Cardiology, University Hospital of Lausanne and University of Lausanne, Lausanne, 5Cardiology Division, University Hospitals of Geneva, Geneva, 6Service of Cardiology and Cardiac MR center, 7Service of Cardiology and Cardiac MR Center, University Hospital of Lausanne and University of Lausanne, Lausanne, Switzerland
Introduction: 2D phase-contrast cardiac magnetic resonance (2D PC-CMR) is considered as gold-standard for blood flow quantification in congenital heart disease (CHD). Accurate planning and performing of multiple 2D PC-CMR acquisitions during one CMR scan is time-consuming and challenging in e.g. young children. 4D PC-CMR allows easy acquisition of a single 3D volume and retrospective quantification of blood flow in any vessel or plane of interest, thus overcoming many of the difficulties of 2D PC-CMR. This study compares 2D vs. 4D PC-CMR derived flow in major blood vessels and their internal consistency.
Methods: 2D PC-CMR scans were planned on balanced steady-state free precession sequences in three orthogonal planes and acquired during free breathing with 2-3 averages. 4D PC-CMR was performed using a free-breathing, prototype navigator-gated 3D cine phase-contrast CMR sequence with three-directional velocity-encoding. Blood flow in the ascending aorta (AA), the main pulmonary artery (MPA), the superior vena cava (SVC), the descending aorta (DA), the right and the left pulmonary artery (RPA, LPA), as well as the Qp:Qs (calculated as MPA flow/AA flow) were compared between 2D and 4D PC-CMR by Bland-Altman plot analyses. The internal consistency was evaluated by determining the correlations of MPA vs. RPA+LPA and MPA vs. AA (where there was no shunt) flows on 2D PC-CMR and MPA vs. RPA+LPA, MPA vs. right pulmonary veins (RPV)+left pulmonary veins (LPV), RPA+LPA vs. RPV+LPV and MPA vs. AA flows on 4D PC-CMR.
Results: 31 patients were included for analysis (mean age 25, range 2-60 years). Diagnoses included a wide range of simple to complex CHD lesions like singe ventricle after Fontan palliation. Duration of acquisition of one 2D PC-CMR flow was 1-2 minutes whereas duration of the total 4D PC-CMR acquisition was about 4 minutes. 2D PC-CMR flows correlated significantly: MPA vs. RPA+LPA, r = 0.87, p<0.0001; MPA vs. AA, r = 0.62, p<0.01 as well as on 4D PC-CMR: MPA vs. RPA+LPA, r = 0.91, p<0.0001; MPA vs. RPV+LPV, r = 0.79, p<0.000001; RPA+LPA vs. RPV+LPV, r = 0.75, p<0.000001; MPA vs. AA, r = 0.72, p<0.0001. Results of the Bland-Altman analyses are shown in Table P97-1.
Table P97-1. Differences between blood flow measurements by 4D PC-CMR vs. 2D PC-CMR using Bland-Altman plot analyses
4D vs. 2D flow
Bias ± Standard deviation (lower, upper limit of agreement), in l/min/m2
Bias ± Standard deviation (lower, upper limit of agreement), in %
Ascending aorta
-0.22 ± 0.32 (-0.86, 0.41)
-7.45 ± 11.57 (-30.12, 15.22)
Superior vena cava
-0.14 ± 0.32 (-0.77, 0.49)
-6.82 ± 26.86 (-59.47, 45.84)
Descending aorta
-0.37 ± 0.32 (-0.99, 0.26)
-20.63 ± 15.78 (-51.56, 10.30)
Main pulmonary artery
-0.22 ± 0.49 (-1.19, 0.75)
-6.68 ± 16.62 (-39.25, 25.89)
Right pulmonary artery
-0.12 ± 0.37 (-0.84, 0.60)
-2.74 ± 23.41 (-48.62, 43.14)
Left pulmonary artery
-0.10 ± 0.30 (-0.69, 0.49)
-4.35 ± 21.06 (-45.62, 36.93)
Qp:Qs
-0.03 ± 0.19 (-0.40, 0.34)
-0.79 ± 16.27 (-32.68, 31.10)
Conclusion: Compared to 2D PC-CMR, 4D PC-CMR allows a faster and more comprehensive quantification of blood flow in CHD patients with a better internal consistency. There are, however, significant differences between 2D and 4D PC-CMR blood flow measurements which should be evaluated prospectively.
P98
Long-term outcome after surgical repair for partial anomalous pulmonary venous connection compared to isolated atrial septal defect closure
M. Touray1, J. Bouchardy1,2, M. Ladouceur3, M. Schwerzmann4, M. Greutmann5, D. Tobler6, H. Gabriel7, R. Engel8, E. Pruvot1, C. Blanche2, N. Sekarski1, T. Rutz1
1Lausanne University Hospital, Lausanne, 2University Hospital of Geneva, Geneva, Switzerland, 3Hôpital Européen Georges Pompidou, Paris, France, 4Inselspital, Bern University Hospital, Berne, 5University Heart Centre Zurich, Zurich, 6University Hospital Basel, Basel, Switzerland, 7Vienna General Hospital, Vienna, Austria, 8Kantonsspital St. Gallen, St. Gallen, Switzerland
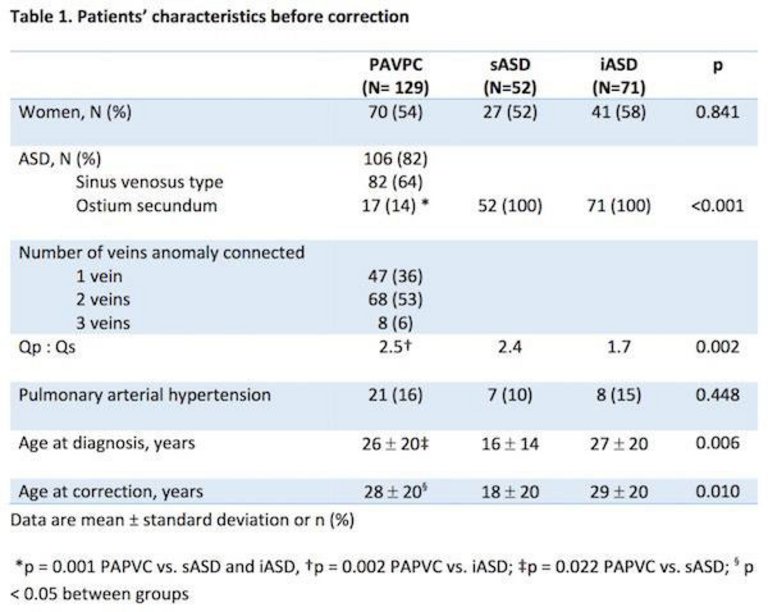
Introduction: Partial anomalous pulmonary venous connection (PAPVC) is a rare congenital heart disease defined by some but not all pulmonary veins aberrantly connected to a systemic vein or to the right atrium with or without an associated atrial septal defect (ASD). The hemodynamic consequences of PAPVC are comparable to a simple secundum ASD. The only curative treatment of PAPVC is a surgical correction, whereas a secundum ASD can also be closed by a percutaneous intervention. This study aims to compare the long-term outcome between adult patients after PAPVC repair and both groups of patients with either surgical or interventionally closed simple secundum ASD (sASD, iASD, respectively), focusing on arrhythmias.
Methods: Clinical, surgical, imaging and invasive data were retrospectively reviewed from 9 centers in Austria, France and Switzerland.
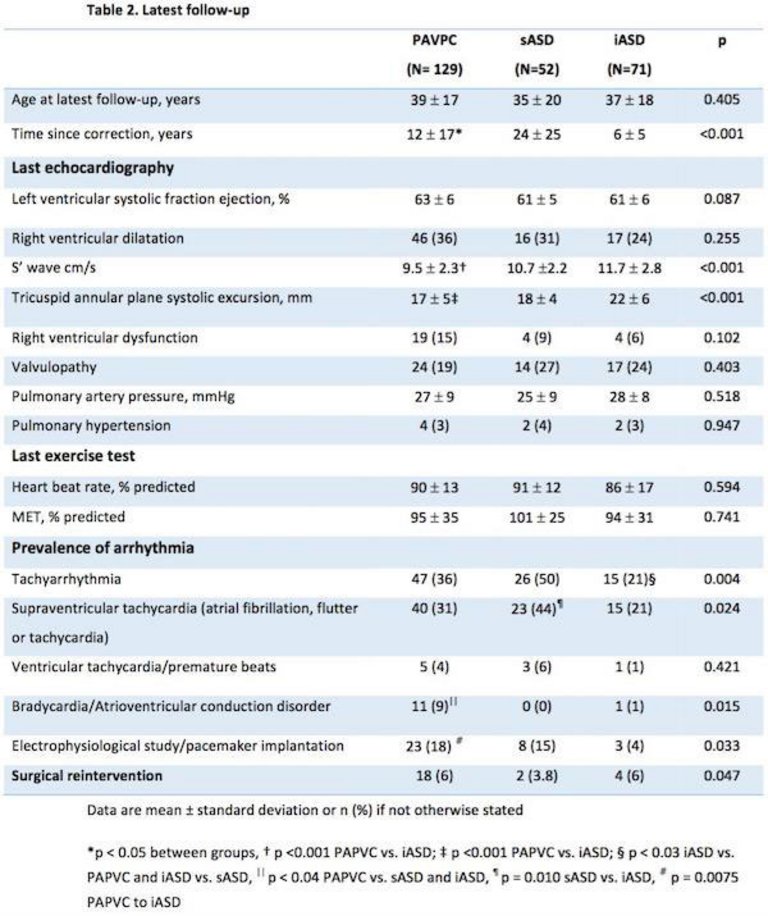
Results: A total of 129 corrected PAPVC, 52 sASD and 71 iASD patients were included (for pre-repair patients' characteristics see figure P98-1). Eighteen percent of patients with PAPVC had an intact atrial septum. sASD patients were diagnosed and operated at younger age than both other groups. PAPVC had a higher Qp:Qs preoperatively than iASD. On last follow-up, PAPVC patients presented a diminished RV longitudinal function (figure P98-2). Exercise capacity, need for cardiac medication and prevalence of symptoms were not different between groups (p >0.1). Supraventricular tachycardia, but not ventricular arrhythmias, were significantly more prevalent in sASD than iASD (figure P98-2). Atrioventricular conduction disorders were significantly more frequent in PAPVC patients (figure P98-2). PAPVC patients required significantly more often an electrophysiological study or a pacemaker implantation than iASD patients (figure P98-2).
Conclusion: Patients requiring surgical repair of PAPVC or sASD display a higher arrhythmia burden than patients corrected by an percutaneous procedure. The higher pre-repair left to right shunt in the surgical corrected groups and/or the surgery itself contribute probably to this finding. A significant number of surgical corrected patients require electrophysiological studies and pacemaker implantation.
Figure
P98-1.
Figure
P98-2.
P99
Long-term outcome in adults with total anomalous pulmonary venous connection: a retrospective multi-center study
M. Touray1, J. Bouchardy1,2, M. Schwerzmann3, M. Greutmann4, D. Tobler5, R. Engel6, H. Gabriel7, E. Pruvot1, C. Blanche2, N. Sekarski1, M. Ladouceur8, T. Rutz1
1Lausanne University Hospital, Lausanne, 2University Hospital of Geneva, Geneva, 3Inselspital, Bern University Hospital, Berne, 4University Heart Centre Zurich, Zurich, 5University Hospital Basel, Basel, 6Kantonsspital St. Gallen, St. Gallen, Switzerland, 7Vienna General Hospital, Vienna, Austria, 8Hôpital Européen Georges Pompidou, Paris, France
Introduction: Total anomalous pulmonary venous connection (TAPVC) is a rare congenital heart disease characterized by all four pulmonary veins aberrantly connected to a systemic vein or the right atrium. The only curative treatment is a surgical correction early after birth.
Due to its rare incidence, data on outcome of these patients is scarce. The aim of the study is to investigate the long-term outcome of survivors after surgical correction with a focus on arrhythmia.
Methods: Clinical, surgical, imaging and invasive data were retrospectively reviewed from patients participating in the Swiss Adult Congenital HEart disease Registry (SACHER).
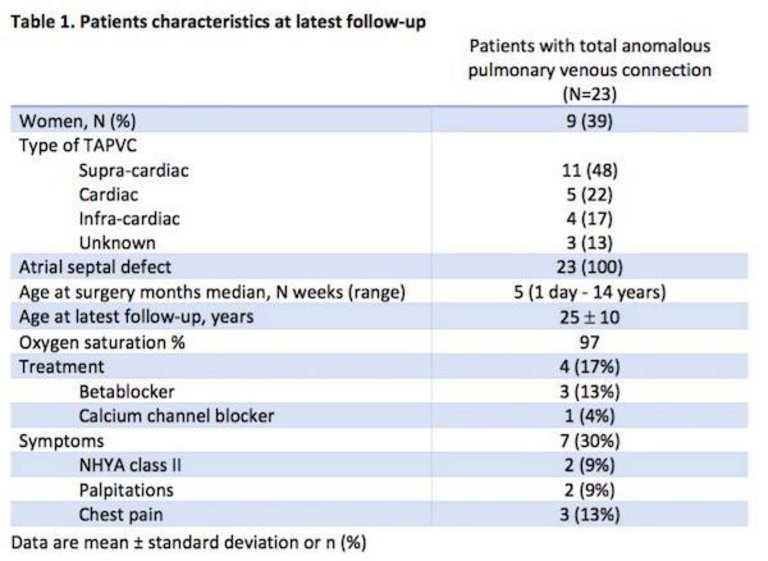
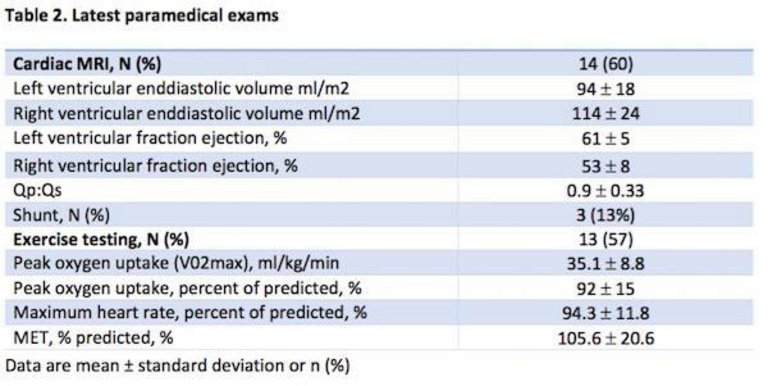
Results: A total of 23 patients were identified (see figure P99-1 for patients' characteristics). Preoperative cardiac catheterization showed an average Qp:Qs of 2.4 ± 1.2. Six (26%) individuals had pulmonary venous obstruction and 8 (23%) developed pulmonary hypertension (PH) prior to surgery. At last follow-up, 6 (26%) patients presented cardiac symptoms (figure P99-1) and no patient had PH or a relevant valvulopathy. Exercise capacity was normal in most patients (figure P99-2). CMR revealed a dilated RV in four (17%) patients and three (13%) had a residual shunt with an mean Qp:Qs of 1.25, in 2 patients due to a single anomalously connected pulmonary vein (figure P99-2).
Holter-ECG revealed arrhythmia in 9 (39%) patients. Six (26%) had atrial fibrillation, flutter or tachycardia and 3 (13%) bradycardic rhythm disorders. Three (13%) patients presented ventricular arrhythmias: two patients showed non-sustained ventricular tachycardia and one patient complex ventricular extrasystoles.
Five (21%) individuals required medical treatment for arrhythmias, three (17%) an electrophysiological study. Two (9%) patients underwent pacemaker implantation within 3 weeks after surgical correction which were removed in both patients after 7 years.
During follow-up, 3 (17%) patients developed pulmonary vein stenosis. Three (17%) patients required a re-intervention, 2 (9%) patients for pulmonary vein stenosis and 1 (4%) individual for an inferior vena cava that was inadvertently redirected to the left atrium during the first operation.
Conclusion: Adult survivors after TAPVC repair present not only supraventricular but also ventricular arrhythmias leading to a significant morbidity. These findings demonstrate the need for a long-term follow for patients after TAPVC repair.