Joint Annual Meeting 2019 of the Swiss Society of Cardiology and the Swiss Society of Cardiac Surgery
O76
Staging classification of cardiac damage according to invasive hemodynamics in patients with severe aortic stenosis undergoing valve replacement
M.T. Maeder1, L. Weber1, M. Buser1, N.F. Ehl1, P.K. Haager1, L. Joerg1, M. Taramasse2, D. Weilenmann1, F. Maisano2, H. Rickli1
1Kantonsspital St. Gallen, St. Gallen, 2University Hospital Zürich, Zurich, Switzerland
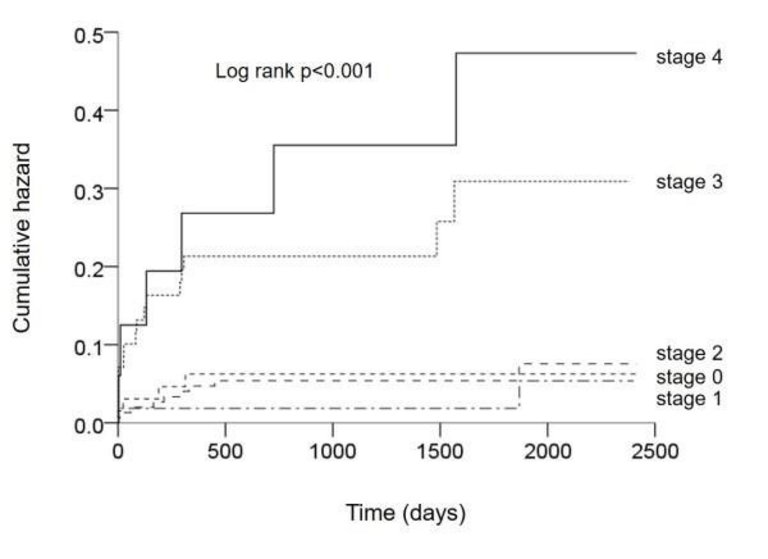
Background: Recently, a staging classification of cardiac damage in aortic stenosis (AS) based on echocardiographic measurements has been shown to provide prognostic information after aortic valve replacement (AVR; Généreux P et al. Eur Heart J 2017). We aimed to validate this principle by creation of an analogous five stage classification based on invasive hemodynamics.
Methods: We studied 422 patients (age 75±10 years, 59% males) with severe AS [indexed aortic valve area (iAVA) 0.41±0.13 cm2/m2] undergoing AVR with complete pre-AVR invasive hemodynamics. The five stages of cardiac damage were defined as follows: stage 0: no cardiac damage: absence of any of the following criteria, stage 1: left ventricular damage: left ventricular end-diastolic pressure >15 mmHg, stage 2: left atrial damage: mean pulmonary artery wedge pressure >15 mmHg, stage 3: pulmonary vascular damage: pulmonary vascular resistance >3 Wood units and/or invasively assessed systolic pulmonary artery pressure >60 mmHg, stage 4: right ventricular damage: mean right atrial pressure >15 mmHg. Patients were hierarchically classified in a given stage (worst stage) if the criterion was met for that stage.
Results: Sixty-seven (16%) patients were classified as stage 0, 113 (27%) as stage 1, 152 (36%) as stage 2, 73 (17%) as stage 3, and 17 (4%) as stage 4. There was a progressively lower cardiac index from stage 0 to stage 4 (analysis of variance p<0.001). Mortality at 30 days after surgical (n = 295) or transcatheter (n = 127) AVR in patients in stages 0 to 4 was 3.0%, 2.7%, 1.3%, 9.6%, and 11.8% (p = 0.008). After a median (interquartile range) follow-up of 3.8 (2.7-5.2) years, mortality was highest in patients in stage 4 [hazard ratio (95% confidence interval) 6.17 (1.74-21.89) compared to stage 0; p = 0.005] and stage 3 [hazard ratio (95% confidence interval) 4.17 (1.39-12.49) compared to stage 0; p = 0.01] while mortality did not differ between patients in stages 0 to 2 (Figure O76-1).
Conclusions: The present data show the prognostic importance of a staging system of cardiac damage fully based on invasive hemodynamic parameters in patients with severe AS undergoing AVR. Importantly, patients with evidence of pulmonary vascular disease and/or significant right ventricular dysfunction had a markedly increased risk of death, whereas patients with left ventricular and/or left atrial damage but without pulmonary vascular involvement had similar outcomes as patients without cardiac damage.
Figure
O76-1.
O77
Outcomes of transcatheter tricuspid valve intervention (TTVI) in patients with pacemaker or defibrillator leads: data from the TriValve Registry
M. Taramasso, on behalf of TRIVALVE Investigators
University Hospital Zürich, Zurich, Switzerland
Background: The interference of a trans-tricuspid cardiac implantable electronic devices-leads (CIED) may contribute to the mechanism of TR. Feasibility and efficacy of TTVI in presence of a CIED is unclear.
Methods: Data from TriValve Registry on patients undergoing TTVI with different CIED were analyzed. The study population consisted of 470 patients with severe symptomatic TR treated at 21 centres between 2015 and 2018. The association of CIED and outcomes were assessed.
Results: Pre-procedural transvalvular lead was present in 121/470 patients (25.7%) undergoing TTVI. An interference of the CIED contributing to TR was described in 44% of the cases. As compared to patients without a transvalvular lead (no-CIED group), patients having a tricuspid lead (CIED group) had similar clinical risk profile (EuroScore II 10.8±10% Vs 10.3±11.5 -p = 00.6), but were more symptomatic (NYHA class III-IV in 95.9% vs 92.3% -p = 0.04), had higher level of NT-proBNP (7920±1079 pg/ml Vs 4851±446 pg/gl) and more frequently had at least 1 hospitalisation for RV failure (87,8% Vs 69% -p = 0.0018). CIED patients had larger LVEDD (54±11.6 Vs 49.3±8.5 mm -p = 0.0004) and lower LVEF (43.2±15% Vs 52.4±12% -p<0.0001). No-CIED patients had more severe TR (EROA 0.7±0.6 cm2 Vs 0.58±0.3 cm2, p = 0.02; VC 1.3±1.7 cm Vs 1.0±0.7, p = 0.03), but significantly better RV function (TAPSE 16.7±5 mm Vs 15.9±4 mm, p = 0.04) and higher sPAP (41.6±14.9 mmHg Vs 37.5±15.3 mmHg, p = 0.008). The most frequently used TTVI device in CIED group patients was MitraClip (106 patients, 87,6%). Procedural success (defined as device successfully implanted and residual TR ≤2+) was achieved in 80% of no-CIED group and in 78.6% of CIED-group (p = 0.74), with an in-hospital mortality of 2.9% and 3.7%, respectively (p = 0.7). At 30 day, residual TR≤2+ was observed in 70.8% of no-CIED group and in 73.69% of CIED-group (p = 0.6). Symptomatic improvement was observed in both groups (NYHA class I-II at 30 days 66% Vs 65% - p = 0.3). Actuarial survival at 14 months was 75.7±4.3% in no-CIED group and 68.3±7% in CIED-group (p = 0.3).
Conclusions: Compared to no-CIED patients, TR patients with CIED have worse baseline left ventricular function and more symptomatic right heart failure despite preserved right ventricular function and less severe TR. TTVI is feasible in patients with CIED and acute procedural success and short-term clinical outcomes are comparable to those observed in patients without a trans-tricuspid lead.
O78
Single-centre three-year experience with the HeartMate 3 left ventricular assist device
A. Nowacka1, P. Tozzi1, N. Barras2, J. Regamey2, P. Yerly2, R. Hullin2, L. Rosner3, C. Marcucci3, M. Rusca4, P. Eckert4, M. Kirsch1
1Department of Cardiac Surgery, 2Department of Cardiology, 3Department of Anesthesiology, 4Department of Intensive Care, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland
Background: Mechanical circulatory support with a continuous-flow left ventricular assist device (LVAD) has become major therapeutic option for patients with end stage heart failure. The HeartMate 3 (HM3) is a latest generation LVAD using a fully magnetically levitated impella with an artificial pulse, large blood flow gaps to avoid blood stasis and a modular driveline. In our center, this device is used since Nov 2015 and has become our first line device to support end stage heart failure patients.
Methods: We retrospectively reviewed our experience with adult and pediatric patients suffering end-stage heart failure who received a HM3 device between Nov. 2015 and Nov. 2018 in our center. The objective of this descriptive study was to analyze demographic data, clinical characteristic, adverse events and survival of patients supported with the HM3 LVAD.
Results: The HM3 LVAD was implanted in 30 consecutive patients (27 males, mean age 56.0±12.7 years). The series included one pediatric recipient, aged 14 years. Etiology for end stage heart failure included ischemic heart disease [AMI in 5 (17%), ischemic cardiomyopathy in 15 (50%)], dilated cardiomyopathy in 8 (27%) and other causes in 2 (6%), patients. Sixteen (53%) patients had a pre-implant INTERMACS clinical profile of 1 to 3. Mean duration of LVAD support was 12.0±7.5 months (range, 1.4 to 33 months). During follow-up (mean, 15.7±9.9 months; total, 471.5 patient-months), 12 patients (40%) received a heart transplant, 3 patients died while on support (10%), and 15 are still ongoing. Actuarial estimates for survival under support were 92.8±4.9% and 88.0±6.6% at 6 and 12 months after implantation, respectively. Six patients (20%) required post-implant temporary right ventricular support (weaned after 2-10 days). Adverse events included bleeding requiring surgery in 9 (30%), GI bleeding in 4 (13%), LVAD specific infections in 9 (30%), non-LVAD related infections in 13 (43%), ischemic stroke in 4 (13%) patients, and 1 patient (3%) with post-traumatic cerebral bleeding. There were no cases of pump thrombosis or technical malfunction.
Conclusions: The absence of pump thrombosis or technical failure during our three-year experience with the HM3 LVAD confirms its high technical reliability. Added to adequate patient selection, surgical technique, and post-operative follow-up, excellent survival with acceptable burden of adverse events could be achieved, which were similar to those reported in the literature.
O79
Hemodynamic implications of concomitant mitral regurgitation in patients with aortic stenosis undergoing aortic valve replacement
M.T. Maeder1, L. Weber1, M. Buser1, M. Gerhard1, P.K. Haager1, L. Joerg1, M. Taramasso2, D. Weilenmann1, F. Maisano2, H. Rickli1
1Kantonsspital St. Gallen, St. Gallen, 2University Hospital Zürich, Zurich, Switzerland
Figure
O79-1.
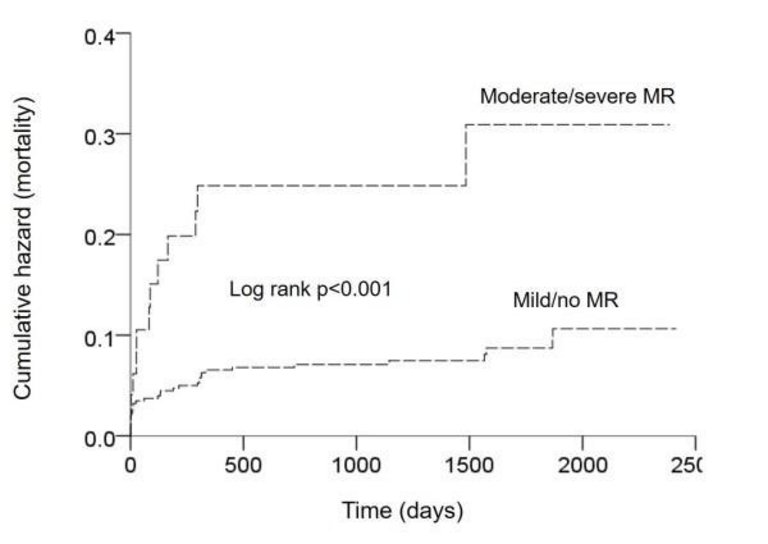
Background: In patients with severe aortic stenosis (AS) undergoing aortic valve replacement (AVR) concomitant moderate or severe mitral regurgitation (MR) has been found to be associated with worse outcomes. In the present study, we compared invasive hemodynamics and mortality in patients with AS with moderate or severe MR to those with mild or no MR as a basis to understand the prognostic importance of significant MR.
Methods: We studied 467 patients (age 74±10 years, 57% males) with severe AS [indexed aortic valve area (iAVA) 0.41±0.13 cm2/m2, left ventricular ejection fraction (LVEF) 57±12%] undergoing pre-AVR right heart catheterization in whom the severity of MR was graded by echocardiography.
Results: Patients with moderate/severe MR (n = 50) were older (79±6 vs. 74±10 years; p = 0.001) and were more symptomatic (NYHA III/IV: 52% vs. 30%; p<0.001) than those with mild/no MR (n = 417). Despite similar AS severity (iAVA: 0.41±0.15 vs. 0.41±0.12 cm2/m2; p = 0.98) those with moderate/severe MR had larger indexed left ventricular end-diastolic diameter (28±9 vs. 24±5 mm/m2), lower LVEF (50±15 vs. 58±11%), larger indexed left atrial area (17±6 vs. 12±3 cm2/m2), higher mean pulmonary artery pressure (34±13 vs. 25±9 mmHg), higher mean pulmonary artery wedge pressure (21±8 vs. 16±8 mmHg; p<0.001 for all) and lower stroke volume index (31±11 vs. 36±10 ml/m2; p = 0.001) than those with mild/no MR. Importantly, patients with moderate/severe MR also had higher pulmonary vascular resistance (3.2±2.0 vs. 2.0±1.2 Wood units; p<0.001), lower tricuspid annular plane systolic excursion (19±5 vs. 21±5 mm; p = 0.02), and higher mean right atrial pressure (8±5 vs. 6±4 mmHg; p = 0.002) than those with mild/no MR. After a median (interquartile range) follow-up of 3.6 (2.6-5.1) years after surgical (n = 330; in 15 patients combined with mitral valve replacement/repair) or transcatheter (n = 137) AVR, patients with moderate/severe MR had worse survival than those with mild/no MR (log rank p<0.001; Figure O79-1)
Conclusions: In patients with severe AS, the presence of moderate or severe MR is marker of a poor hemodynamic profile and markedly increased long-term mortality. Importantly, patients with moderate or severe MR not only have larger left ventricular and left atrial size and higher left-sided filling pressures but also evidence of pulmonary vascular remodeling and right ventricular dysfunction. Thus, in AS patients with concomitant MR specific management strategies have to be developed.
O80
Clinical comparative analysis of Bretschneider and St. Thomas cardioplegia solution in mitral valve repair via anterolateral right thoracotomy
C. Mork, O. Reuthebuch, B. Gahl, L. Koechlin, F. Eckstein, M. Grapow
Department of Cardiac Surgery, University Hospital Basel, Basel, Basel, Switzerland
Background: Single dose Cardioplegia is preferred in minimal invasive mitral valve surgery to maintain preset visualization. The aim of our study is to compare two widely used crystalloid cardiopleagias Bretschneider (Custodiol®) versus St. Thomas crystalloid cardioplegia in patients who underwent mitral valve repair via small anterolateral right thoracotomy by performing a retrospective analysis.
Material and methods: From January 2012 until December 2019, 182 isolated mitral valve procedures for mitral valve repair via anterolateral right thoracotomy were performed. While 128 patients underwent myocardial protection with Bretschneider cardioplegia (Custodiol®), 54 patients received St. Thomas cardioplegia. Primary efficacy endpoint was peak postoperative high-sensitivity cardiac troponin (hs-cTnT) during hospitalization. Secondary endpoints were peak creatine kinase- myocardial type (CK-MB) and creatine kinase (CK) as well as safety outcomes. We used inverse probability of treatment weighting (IPTW) in order to adjust for confounding by indication, including age, female gender, logistic EuroSCORE and hypertension as covariates into the propensity model. We trimmed the tails of the propensity score, as the corresponding records are suspicious of residual confounding and calculated standardized differences to assess comparability of treatment groups after IPTW.
Results: Trimming did not cause substantial patient loss and treatment groups turned out comparable after IPTW with respect to patient characteristics such as age, female gender, body mass index (BMI) and comorbidities. The primary endpoint peak hs-cTnT showed a significant difference between Bretschneider (geometric mean 725 mg/L, reference range 613-858 mg/L) and St. Thomas (643 mg/L, reference range 538-768 mg/L, p = .027). Peak CK-MB (geometric mean after Bretschneider 45 µg/l, reference range 40-52, St. Thomas: 35 µg/l, reference range 30-42, p = .028) and CK (geometric mean after Bretschneider 1489U/l, reference range 1326-1671, St. Thomas: 1242 U/l, reference range 1043-1478, p = .036) showed the same pattern. We did not see any difference with respect to postoperative complications between treatment groups after IPTW.
Conclusion: Use of St. Thomas cardioplegia was associated with lower postoperative peak levels of all cardiac markers that reflect cardiac ischemia such as hs-cTnT, CK and CK-MB as compared to Bretschneider in propensity-weighted treatment groups.
O81
Safety and efficacy of transcatheter aortic valve implantation with continuation of oral anticoagulation
S. Toggweiler1, M. Brinkert1, L. Keller2, N. Moriyama3, M. Bossard1, M. Laine3, F. Cuculi1, R. Kobza1, F. Nietlispach2
1Herzzentrum, Luzerner Kantonsspital, Luzern, 2Cardiology, University Hospital Zürich, Zurich, Switzerland, 3Cardiology, Helsinki University Central Hospital, Helsinki, Finland
Introduction: Up to one third of patients undergoing transcatheter aortic valve implantation (TAVI) have an indication for long-term oral anticoagulation. The optimal periprocedural medical management of such patients is unknown.
Methods: Consecutive patients on oral anticoagulation therapy with either a vitamin K antagonist or a direct oral anticoagulant who underwent transfemoral TAVI at three European centers between 2015 and 2018 were enrolled. Oral anticoagulation was either stopped 2-4 days prior to TAVI and restarted after TAVI or continued throughout the procedure.
Results: Out of 1370 consecutive patients undergoing transfemoral TAVI, 371 patients had an indication for oral anticoagulation (atrial fibrillation in 95%). A total of 186 patients underwent TAVI with continuation and 185 patients with interruption of anticoagulation. CHA2DS2-VASc-Score was high in both groups with 5.1 ± 1.5 points. At 30 days, the rates of major or life-threatening bleedings were 19 (10.2%) versus 20 (10.8%) among patients with continuation and with interruption of anticoagulation, respectively (p = 0.71). Major vascular complications occurred in 16/186 patients with continuation of anticoagulation as compared with 19/185 patients with interruption (8.6% vs 10.3%, p = 0.86). Ischemic strokes were rare and occurred in 1 (0.55%) vs 6 (3.24%, p = 0.12), respectively. Mortality at 30 day was 4.3% vs 2.2%, respectively (p = 0.38). Kaplan Meier estimates of survival at 1 year were 91% in both groups (log rank p = 0.90).
Conclusion: Patients with continuation of oral anticoagulation throughout TAVI did not have more bleeding or vascular complications. There was a signal towards lower stroke rates in patients with continuation of anticoagulation. Based on the results of this relatively small study, simplifying the TAVI procedure protocols with continuation of oral anticoagulation throughout the procedure appears to be safe and may help to prevent periprocedural strokes during TAVI.
O82
Exercise hemodynamics on LVAD support: poor left ventricle unloading despite normal hemodynamics at rest
J. Regamey1, N. Barras1, P. Tozzi2, M. Kirsch2, R. Hullin1, P. Yerly1
1Département Coeur-Vaisseaux - Service de Cardiologie, 2Département Coeur-Vaisseaux - Service de Chirurgie Cardiaque, CHUV, Lausanne, Switzerland
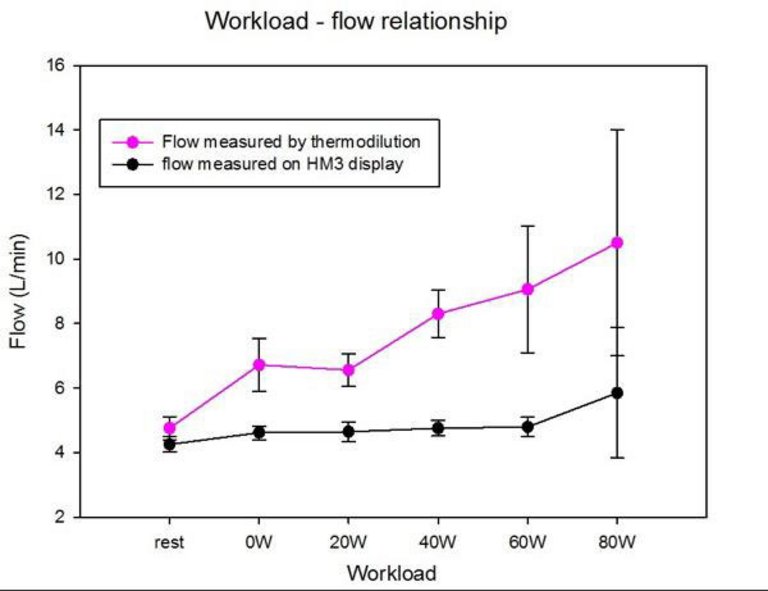
Introduction: Although NYHA class improvement has been reported after LVAD implantation in advanced heart failure, peak VO2 often remains reduced, which contrasts with cardiac output (CO) and filling pressure improvement at rest. One reason may be insufficient unloading of the left ventricle during exercise. To test this hypothesis, we invasively explored exercise hemodynamics in 5 successive patients on LVAD (Heartmate 3, Abbott®), taken to routine right heart catheterization (RHC) for pump speed optimization.
Method: Patients (age 58±11, 4 males, 4 with ischemic cardiomyopathy, in stable NYHA class II [n = 3] or III [n = 2] and no congestion) were on support for 528±338 days. RHC (Swan-Ganz catheter in jugular vein) and echocardiography were performed simultaneously at rest in supine position. Pump speed was adapted in order to achieve pulmonary artery wedge pressure (PAWP) <15 mmHg and right atrial pressure (RAP) <8 mmHg, with interventricular septum in median position and intermittent aortic valve opening if possible. Symptom-limited exercise was performed on a cycloergometer in a semi-supine position with stepwise 20W workload increases. CO was measured by thermodilution (TD) with 2-3 measures at each step. PA pressure (Ppa) curves were recorded at each step. Systolic, diastolic, mean Ppa and PAWP were considered as the average between inspiration and expiration. LVAD pump flow was simultaneously reported.
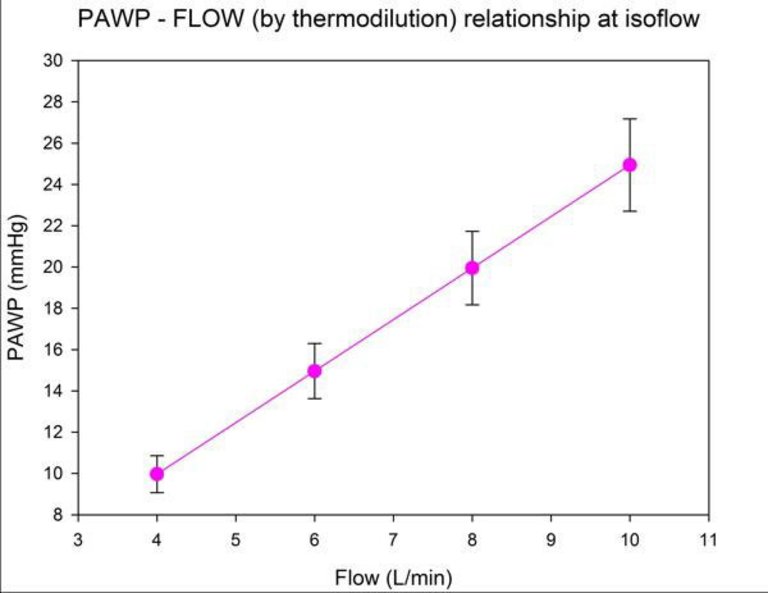
Results: All patients had normal filling pressures (PAWP = 10±1 and RAP = 5±2 mmHg) at rest with pump speed at 5620±311 rpm. TD-assessed CO (5.36±1.52 L/min at rest) increased by 50.1±11.2 mL/min/W to reach 9.69±2.52 L/min at maximal exercise (P = 0.0018). By contrast, LVAD pump flow (4.48±0.45 L/min) raised only by 14.1±7.6 mL/min/W without significant increase (5.17±1.06 L/min; P = 0.06) at maximal exercise (Fig. O82-1). PAWP sharply raised to 22.8±4.5 mmHg at maximal exercise (P = 0.001 as compared to rest), with a PAWP-TD flow relationship of 2.49±0.31 mmHg/L/min (Fig. O82-2).
Conclusion: This small study shows that flow through LVAD marginally increases at exercise, which leads to severe impairment of LV filling pressure and PAWP-flow relationships similar to those observed with heart failure and preserved ejection fraction. Poor LV unloading at exercise may contribute to persistent exercise limitation after LVAD implantation.