Joint Annual Meeting 2019 of the Swiss Society of Cardiology and the Swiss Society of Cardiac Surgery
O45
Diabetes and entry glucose levels both determine outcomes in acute coronary syndromes
T.F. Lüscher1, P. Winzap2, A. Davies3, S. Obeid4, M. Roffi5, A. Von Eckardstein6, R. Klingenberg7, F. Mach5, L. Raeber8, S. Windecker8, C. Templin4, F. Nietlispach4, O. Muller9, D. Nanchen10, C. Matter4, SPUM ACS and Inflammation
1Imperial College | Cardiology | Royal Brompton Hosapital, Royal Bropmton and Harefield Hospitals, London, United Kingdom, 2Center for Molecular Cardiology, University of Zurich, Schlieren, 3Heart Division, Imperial College, London, 4Cardiology, University of Zurich, Zurich, 5Cardiology, Université de Geneve, Geneve, 6Clinical Chemistry, University of Zurich, Zurich, Switzerland, 7Cardiology, Kerckhoff Klinik, Bad Nauheim, Germany, 8Cardiology, Inselspital Bern, Berne, 9Cardiologie, Centre Hospitalier Universitaire Vaudois, Lausanne, 10Cardiologie, Centre Hospitalier Universitaire Vaudois, Policlinique Medicale, Switzerland
Background: Cardiovascular diseases (CVDs) remain the main cause of deaths worldwide, primarily due to acute coronary syndromes (ACS). Diabetes and the metabolic syndrome are major risk factors for such events. The prevalence of diabetes has been estimated at 10% in adults aged over 25 and more than half of diabetics are expected to die from cardiovascular problems. Here we investigated the impact of hyperglycaemia and diabetes on outcomes in a contemporary cohort of patients with ACS.
Methods: The prospective SPUM-ACS cohort enrolled 2,168 patients with ACS, out of which 2,034 underwent a percutaneous coronary intervention (PCI; 93.8%). Outcomes were reported at 30 and at 365 days. Patients were grouped according to history of diabetes, admission glucose and body mass index (BMI). The primary endpoint was major adverse cardiac events (MACE). Secondary endpoints included all-cause death, revascularisation, bleeding and cerebrovascular events. All events were independently adjudicated.
Results: Diabetics experienced significantly more MACE and strokes and had a higher mortality. Patients with glucose levels of >6 mmol/L at presentation had higher risk of death, stroke and MACE at one year, irrespective of diabetic status. More revascularization procedures were performed in diabetics at 30 days, but not at one year. When grouping patients into quartiles based on entry glucose levels, quartile 4 with glucose levels of >7.7 mmol/L showed the highest MACE rate, while quartile 2 with glucose levels of 5.51-6.3 mmol/L had the lowest risk of MACE. There was a non-significant trend towards higher MACE and mortality in diabetics and non-diabetics with elevated glucose levels. Of all diabetics, those with BMI <25 had the highest MACE, while non-diabetics with BMI <25 had higher mortality at 1 year.
Conclusion: In a large, prospective, independently adjudicated population of patients with ACS undergoing PCI, a history of diabetes was associated with increased risk of MACE. Both diabetics and non-diabetics with elevated glucose on presentation with ACS have significantly increased risk of MACE. Obesity is a protective factor in terms of risk of MACE in both diabetics and non-diabetics.
O46
Prognostic value of novel renal and inflammatory biomarkers in acute coronary syndromes: a multi-marker strategy involving galantine-3, cystic C and neutrophil gelatinase-associated lipocalin
S. Obeid1, N. Yousif1, A. Davies2, R. Loretz1, L. Saleh3, D. Niederseer1, F. Mach4, B. Gencer4, L. Räber5, S. Windecker5, C. Templin1, F. Nietlispach1, D. Nanchen6, N. Rodondi5, O. Muller7, A. Von Eckardstein3, C.M. Matter1, T.F. Lüscher8
1University Heart Centre Zurich, Zurich, 29Royal Brompton and Harefield Hospitals and Imperial College, London, 3Institute of Clinical Chemistry, Zurich, 4Hopital Universitaire de Geneve, Geneva, 5University Hospital Bern, Berne, 6Department of Ambulatory Care and Community Medicine, University of Lausanne, 7Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland, 88Center for Molecular Cardiology, University of Zurich, Switzerland: 9Royal Brompton and Harefield Hospitals and Imperial College, London, United Kingdom., London, United Kingdom
Introduction: Cystatin C, neutrophil gelatinase-associated lipocalin (NGAL) and galectin-3 emerged as biomarker candidates to predict cardiovascular outcomes and mortality in the general population as well as in patients with coronary artery (CAD) or renal disease. However, their predictive role and clinical utility in patients with acute coronary syndromes (ACS) alone and in combination remains to be determined.
Methods and Results: Cystatin C, NGAL, and galectin-3 were measured in plasmas of 1'832 patients at the time of presentation with ACS requiring percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). The primary outcomes were major adverse cardiac and cerebrovascular events (MACCE) and all-cause mortality after 1 year and occurred in 192 (10.5%) and 78 (4.3%) of patients, respectively. Galectin-3 (all-cause mortality: HR = 1.027 [95%CI(1.011-1.043);p = 0.001], MACCE: HR = 1.025 [95%CI(1.012-1.037);p<0.001]) but neither cystatin C nor NGAL emerged as independent predictor of both MACCE and death. The risks were particularly high in the highest quartile of galectin-3. The integration of galectin-3 into the GRACE score improved the prediction of MACCE and all-cause mortality significantly. The areas under the receiver operator characteristics curves increased from 0.6701 to 0.6932 for MACCE (p = 0.0474) and from 0.804 to 0.8199 for all-cause mortality (p = 0.0197).
Conclusions: In ACS patients, galectin-3 is a potent and independent predictor of clinical outcome beyond currently used measures and should be considered in future risk scores for the management of ACS patients.
O47
Diagnosis of acute myocardial infarction in the presence of left bundle-branch block
T. Nestelberger1, L. Cullen2, B. Lindahl3, T. Reichlin4, R. Twerenbold1, L. Koechlin1, J. Boeddinghaus1, M. Rubini1, J. Greenslade2, S. Osswald1, C. Mueller1
1Unispital Basel, Basel, Switzerland, 2Royal Brisbane & Women's Hospital, Hersten, ACT, Australia, 3Department of Medical Sciences,, University of Uppsala, Uppsala, Sweden, 4Bern University Hospital, Berne, Switzerland
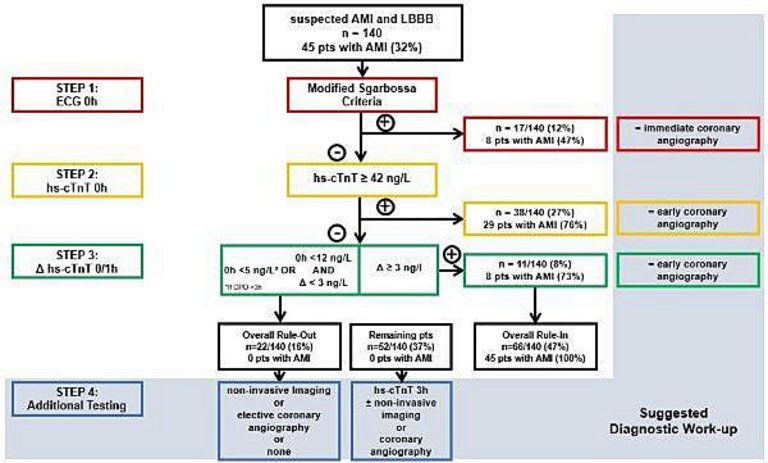
Introduction: Patients with suspected acute myocardial infarction (AMI) in the setting of left bundle branch block (LBBB) present an important diagnostic and therapeutic challenge to the clinician.
Methods: We prospectively evaluated incidence of AMI, and diagnostic performance of specific electrocardiographic (ECG) and high-sensitivity cardiac troponin (hs-cTn) criteria in patients presenting with chest discomfort to 26 emergency departments in three international, prospective, diagnostic studies. Presence of LBBB, ECG criteria, and final diagnoses were centrally adjudicated by two independent cardiologists using the fourth universal definition of myocardial infarction.
Results: Among 8830 patients, LBBB was present in 247 patients (2.8%). AMI was the final diagnosis in 30% of patients with LBBB, with similar incidence in those with known LBBB versus those with presumably new LBBB (29% vs 35%, p = 0.42). ECG criteria had low sensitivity (1-12%), but high specificity (95-100%). The diagnostic accuracy as quantified by the receiver-operating-characteristics curve of hs-cTnT and hs-cTnI concentrations at presentation (AUC 0.91; 95%CI 0.85-0.96 and 0.89; 95% CI 0.83-0.95) as well as that of their 0/1h and 0/2h changes was very high. A diagnostic algorithm combining ECG criteria with hs-cTnT/I concentrations and their absolute changes at 1h or 2h derived in cohort 1 (45 of 45 (100%) of patients with AMI correctly identified), showed high efficacy and accuracy when externally validated in cohort 2&3 (28 of 29 patients, 97%).
Conclusion: Most patients presenting with suspected AMI and LBBB will be found to have diagnoses other than AMI. Combining ECG criteria with Hs-cTn testing at 0/1h or 0/2h allows early and accurate diagnosis of AMI in LBBB (Figure O47-1).
Figure
O47-1.
O48
Optimal timing of invasive coronary angiography following NSTEMI
T. Mahendiran1, D. Nanchen2, D. Meier1, B. Gencer3, R. Klingenberg4, L. Räber5, D. Carballo3, C. Matter5, T. Lüscher6,7, S. Windecker8, F. Mach3, N. Rodondi9,10, O. Muller1, S. Fournier1
1Department of Cardiology, Lausanne University Center Hospital, 2Center for Primary Care and Public Health (Unisanté), University of Lausanne, Lausanne, 3Department of Cardiology, Geneva University Hospitals, Geneva, Switzerland, 4Department of Cardiology, Kerckhoff Klinik, Bad Nauheim, Germany, 5Department of Cardiology, University Hospital of Zurich, 6Center for Molecular Cardiology, University of Zurich, Zurich, Switzerland, 7Imperial College and Royal Brompton & Harefield Hospitals, London, United Kingdom, 8Department of Cardiology, 9Department of General Internal Medicine, Inselspital, Bern University Hospital, University of Bern, 10Institute of Primary Health Care (BIHAM), University of Bern, Berne, Switzerland
Introduction: Current guidelines recommend angiography within 24 hours of hospitalisation for patients with non-ST elevation myocardial infarction (NSTEMI). The recent VERDICT study found that angiography within 12 hours of hospitalisation was associated with improved cardiovascular outcomes among high-risk patients. We aimed to obtain a real-world perspective of the impact of angiography timing on one-year outcomes of patients admitted with NSTEMI.
Methods: Data was obtained from the SPUM-ACS registry, a cohort of consecutive patients hospitalised with acute coronary syndromes in four university hospitals in Switzerland between 2009 and 2017. Patients without a door-to-catheter (DTC) time and those with life-threatening features were excluded. Cox proportional hazards models evaluated the impact of DTC time on the primary endpoint, defined as one-year major adverse cardiovascular events (MACE: cardiovascular mortality, myocardial infarction, stroke), and on one-year all-cause mortality.
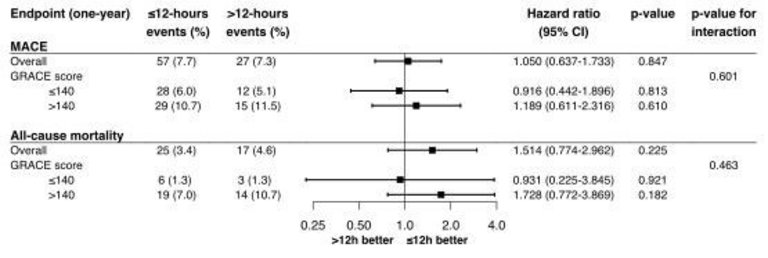
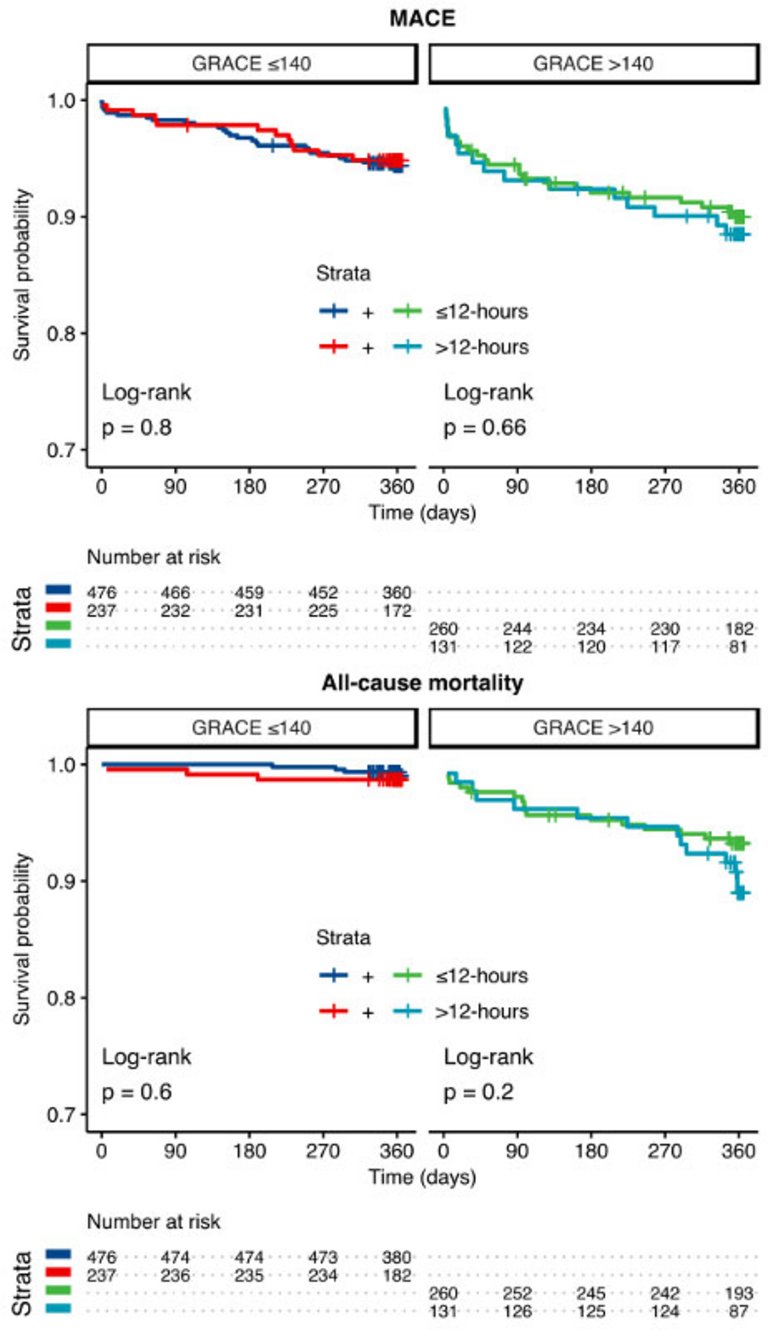
Results: Of 2'672 NSTEMI patients, 1'832 met the inclusion criteria. Among them, 1'464 patients underwent angiography within 12 hours of admission (12h group) while 368 patients underwent angiography between 12 and 24 hours (12-24h group). After 2:1 propensity score matching, 736 patients from the 12h group and 368 patients from the 12-24h group were deemed equivalent in terms of main baseline clinical characteristics. Multiple logistic regression identified admission out-of-hours (night or weekend) as the most significant factor associated with delayed angiography. Cox models found no significant association between early angiography and one-year MACE (12h group: n = 57 (7.7%) vs. 12-24h group: n = 27 (7.3%), HR: 1.050, 95% CI 0.637- 1.733, p = 0.847), or one-year all-cause mortality (12h group: n = 25 (3.4%) vs. 12-24h group: n = 17 (4.6%), HR: 1.514, 95% CI 0.774- 2.962, p = 0.225) (Figure O48-1). After stratification based on GRACE score (>140 vs. ≤140), there was no significant difference in one-year MACE or one-year all-cause mortality in the 12h group compared with the 12-24h group (p for interaction = 0.601 and 0.463, respectively) (Figure O48-1 and O48-2).
Conclusion: In an unselected real-world cohort of NSTEMI patients, angiography within 12 hours of hospitalisation was not associated with improved one-year outcomes when compared with angiography between 12 and 24 hours, even among patients with an elevated GRACE score.
Figure
O48-1. Hazard ratios for one-year endpoints in overall population and after stratification by GRACE score.
Figure
O48-2. Kaplan-Meier analyses stratified by door-to-catheter time and GRACE score.
O49
Predictors for a prolonged time from first medical contact to revascularization
O. Roux1, S. Schukraft2, S. Lehmann2, M. Togni2, J.-C. Stauffer2, J.-J. Goy2, V. Ribordy3, G. Baeriswyl2, A. Attinger2, Z. Kallinikou2, S. Puricel2, S. Cook2
1Service de Cardiologie, CHUV, Lausanne, 2Service de Cardiologie, 3Service des Urgences, University Hospital Fribourg, Fribourg, Switzerland
Introduction: Delays in the care of acute ST-elevation myocardial infarction (STEMI) are associated with increased morbidity and mortality. We sought to find the predictors and the consequences of prolonged first medical contact to revascularization time (FMC-R).
Methods: We analyzed data from the Fribourg STEMI Fast Track Registry (EVALFAST). Starting in June 2008, all patients admitted via the Fast Track managed care system were prospectively enrolled. Relevant patient and procedural data were prospectively collected. Clinical follow-up was performed by phone or clinic visit.
Patients were divided into 2 groups: Patients with a FMC-R interval <90 minutes (short) and those with a FMC-R delay of ≥ 90 minutes (long). Binary logistic regression was performed to find predictors for a FMC-R delay of ≥ 90 minutes.
The primary clinical endpoint was the occurrence of MACE at 3 years. MACE was defined as cardiac death, myocardial infarction or repeat revascularization. Secondary clinical endpoints were death and stent thrombosis at 3 years. Clinical outcome was compared between the 2 patient groups (short vs. long) using Cox regression.
Results: Of 406 patients enrolled from 2008 through 2014, 187 (46%) were treated with a short delay and 219 (54%) with a long delay. Mean age was 63±12 years (short: 61±12 vs. long: 65±12, p = 0.001) and 75% (n = 306) were men (short: 78% vs. long: 74%, p = 0.36).
Age at presentation was the solely predictor associated with long delay. The likelihood of a prolonged delay increased with growing age (per additional year: OR 1.03; 95% CI 1.01-1.05, p = 0.001).
The primary clinical outcome occurred in 15% (n = 28) in the short group and in 25% (n = 54) in the long group (p = 0.02). This difference was driven by numerically higher rates of cardiac death (p = 0.08) and the need of repeat revascularization (p = 0.08).
Conclusion: Age delays revascularization after first medical contact in patients with STEMI. Patients with short waiting period have significantly lower MACE rates at 3 years.
O50
Temporal trends in latecomer ST-segment elevation myocardial infarction patients: insights from the AMIS Plus Registry 1997-2017
M. Roberto1, D. Radovanovic2, L. Biasco1, A. Quagliana1, P. Erne2, H. Rickli3, G. Pedrazzini1, M. Moccetti1, on behalf of AMIS Plus Investigators
1Cardiology Department, Cardiocentro Ticino, Lugano, 2AMIS Plus Data Centre, Epidemiology, Biostatistics and Prevention Institute, University of Zurich, Zurich, 3Cardiology Department, Cantonal Hospital, St. Gallen, Switzerland
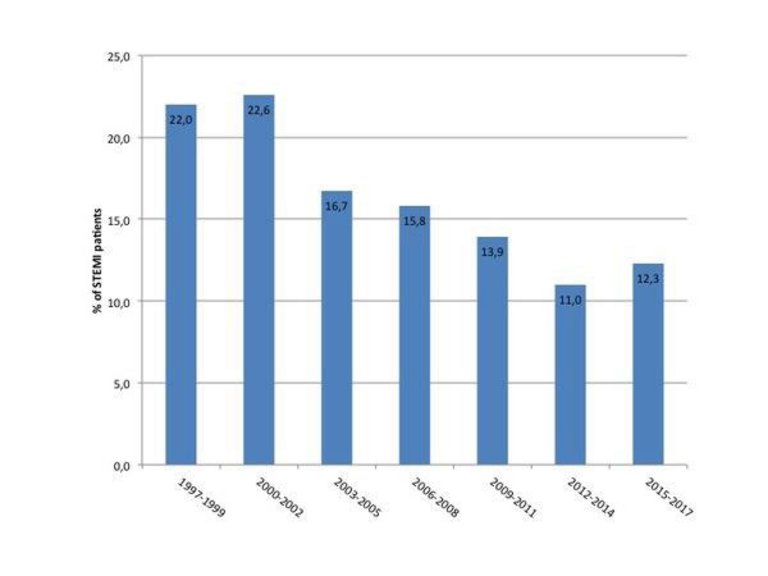
Introduction: A relevant proportion of patients experiencing ST-segment elevation myocardial infarction (STEMI) has a late presentation after symptoms onset. Temporal trends deriving from a large real-word scenario for this subgroup of patients are lacking.
Method: All STEMI patients included in the AMIS Plus Registry from January 1997 to December 2017 were included and patient-related delay was assessed: 27 231 patients were available for the final analysis. STEMI patients were classified as early or latecomers according to patient-related delay (≤ or >12 hours, respectively).
Results: 22 928 patients were earlycomers (84%) and 4303 patients were classified as latecomers (16%). Across the study period we observed a significant decrease in prevalence of late presentation from 22% to 12.3% (p <0.001, Figure O50-1). In latecomer STEMI patients there was a gradual uptake of evidence-based pharmacological treatments with an increase in discharge prescription of P2Y12 inhibitors from 6% to 90.7% (p <0.001). Similarly, a marked increase in percutaneous coronary intervention (PCI) rate was observed (12.1-86.6%; p <0.001). Across this 20-year period, in-hospital mortality was reduced to a third (to an absolute rate of 4.5%, p <0.001) and a significant reduction in prevalence of both cardiogenic shock (14.6-4.3%) and re-infarction (5.4-0.2%) during the index hospitalisation was observed (p <0.001 for both variables). Length of hospitalisation in acute care facilities significantly decreased from 10 (6,14) days to 4 (1,7) days (p <0.001). At multivariate analysis, PCI had a strong independent protective effect toward in-hospital mortality (odds ratio 0.3, 95% confidence interval 0.187 to 0.480).
Conclusion: The present study provides a comprehensive picture of temporal trends in late presentation in STEMI over the last 20 years in Switzerland. During the study period in latecomer STEMI population there was a gradual uptake of evidence-based pharmacological treatments and a marked increase in PCI rate. In-hospital mortality was reduced to a third (to an absolute rate of 4.5%) and this reduction seems to be mainly associated with the increasing implementation of PCI.
Figure
O50-1.
O51
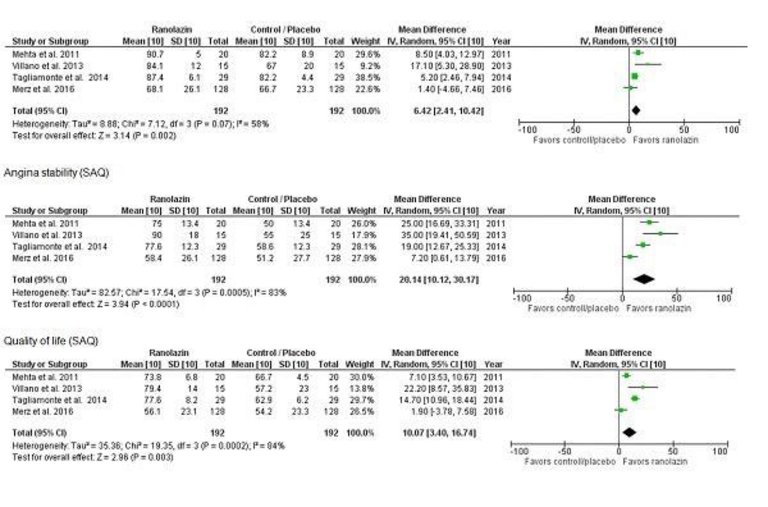
Ranolazine for coronary microvascular dysfunction
T. Kofler1, S. Hess1, F. Moccetti1, S. Aeschbacher2, S. Stämpfli1, F. Cuculi1, S. Toggweiler1, R. Kobza1, M. Bossard1
Introduction: Coronary microvascular dysfunction (CMD) is common cause of angina and exercise intolerance among patients without obstructive coronary artery disease. Recent studies indicate that afflicted patients have a worse prognosis. Current evidence evaluating the clinical efficacy of ranolazine, a late sodium channel blocker, for treatment of CMD remains controversial. To conduct a systematic review and meta-analysis including randomized studies evaluating the effect of ranolazine versus placebo/ standard treatment among CMD patients.
Methods: Medline; Cochrane central, and Embase databases were independently researched by two investigators. Randomized trials from 1975 to February 2019 testing ranolazine versus placebo or standard therapy in patients with CMD were evaluated. Endpoints of interest was change in angina (measured by the Seattle angina questionnaire (SAQ), Clinical outcomes and adverse drug reaction were also analyzed. Data were combined using random-effects models.
Results: Of 1,591 citations, 4 randomized studies (N = 223) were identified. Median follow up was 6 weeks. In the pooled analysis, patients treated with ranolazine, showed an improvement in SAQ components: including improved angina control, improved physical functioning and better quality of life (as displayed in figure O51-1). However, heterogeneity across the included studies was high (median I2 83%). No clinical adverse events or clinically relevant drug side effects have been reported among included studies during follow-up.
Conclusion: Among patients with CMD, ranolazine seems to improve angina and quality of life. However, it remains unknown if it also improves prognosis. There is a need for prospective trials evaluating its long-term impact on outcome.
Figure
O51-1.
O52
Effect of permanent right internal mammary artery occlusion on right coronary artery collateral function. A randomized controlled trial
M.R. Bigler, M. Stoller, C. Tschannen, R. Grossenbacher, C. Seiler
Cardiology, Inselspital, Bern University Hospital, University of Bern, Berne, Switzerland
Introduction: Extracardiac coronary artery supply via the pericardiophrenic branch of the internal mammary arteries (IMA) has been well documented anatomically. Recently, a proof-of-concept study has found functional relevance of these anastomoses in patients with coronary artery disease (CAD) during a brief right coronary artery (RCA) occlusion. The aim of the present randomized controlled, single-blind trial was to investigate the effect of permanent right IMA (RIMA) occlusion on RCA collateral flow index (CFI) and on the occurrence of angina pectoris. We hypothesized that the change in RCA CFI from baseline to follow-up examination is higher in the group of patients with than without permanent RIMA occlusion.
Methods: One hundred patients with CAD were randomly allocated (1:1) to permanent RIMA device occlusion at baseline or to no RIMA occlusion (sham control group). The primary study endpoint was CFI change in the RCA from baseline to the 6-week follow-up examination. CFI is the ratio between mean coronary occlusive and aortic pressure both subtracted by central venous pressure as obtained during a 1-minute proximal RCA balloon occlusion. RCA CFI was measured at baseline before RIMA occlusion or the sham procedure and at the follow-up invasive exam. At the end of the same occlusion, occurrence of angina pectoris was assessed. Percutaneous coronary intervention (PCI) of the RCA was deferred until after follow-up RCA CFI measurement.
Results: There were 51 patients in the RIMA occlusion (verum) group and 49 patients in the sham control group. PCI in the left coronary territory was performed at baseline for clinical reasons in 27 patients of the verum group and in 25 patients of the sham control group. There were no differences in clinical characteristics at baseline between the groups (age 68±12 years, 88 men). RCA CFI change during the 6 weeks of follow-up was equal to +0.028±0.077 in the verum group and -0.026±0.079 in the sham control group (p = 0.0017). Angina pectoris during CFI measurement had disappeared at follow-up exam in 30% of the verum group and in 2% of the sham control group (p = 0.0013).
Conclusions: Right coronary collateral function is augmented 6 weeks after permanent RIMA occlusion when compared to sham treatment. This manifests as less frequent angina pectoris during myocardial ischemia among patients with RIMA occlusion.
O53
Impact of postoperative hypothermia on outcomes after cardiac surgery
V. Ntinopoulos1, N. Papadopoulos1, A. Haeussler1, D. Odavic1, P. Fodor2, O. Dzemali1
1Department of Cardiac Surgery, Triemli Hospital, 2Intensive Care Unit, Triemli Hospital, Zurich, Switzerland
Introduction: Patients undergoing cardiac surgery are at increased risk for postoperative hypothermia. Even though the physiological derangements caused by hypothermia are well described, there is no overall consensus about its impact on postoperative outcomes. Aim of this study is to assess the effect of postoperative hypothermia on outcomes after cardiac surgery.
Methods: We performed a propensity score matched analysis of the data of 4743 patients who underwent major cardiac surgery in our hospital in the period 01/2007-09/2018. The patients were classified according to their core temperature at intensive-care-unit admission postoperatively to either moderately to severely hypothermic (≤35°C) or mildly hypothermic to normothermic (35.1°C-37.4°C). Between groups differences on baseline characteristics and postoperative outcomes were assessed before and after propensity score matching.
Results: In the unmatched population 446 patients (9.4%) were moderately to severely hypothermic and 4297 (90.6%) mildly hypothermic to normothermic. Using propensity score matching 443 moderately to severely hypothermic patients were matched to 443 mildly hypothermic to normothermic ones. There were no statistically significant differences in the baseline characteristics of the matched population except for patient age. Patients with moderate to severe hypothermia exhibited a statistically significantly higher rate of resternotomy because of bleeding or cardiac tamponade (11.5% vs 5%, p<0.0005), renal replacement therapy (10.8% vs 4.7%, p = 0.001), use of red cell concentrates (mean number of units, 2 vs 0.9, p = 0.001), fresh frozen plasma (mean number of units, 0.4 vs 0.2, p = 0.003), intubation duration (median duration, 10 vs 6 hours, p<0.0005), intensive care unit stay (median stay, 6 vs 4 shifts, p<0.0005) and postoperative stay (mean stay, 13.1 vs 12.1 days, p = 0.025) compared to the mildly hypothermic to normothermic ones.
Conclusions: It is important to avoid postoperative hypothermia in order to improve outcomes after cardiac surgery.
O54
Outcomes in patients with left ventricular non-compaction phenotype and normal ejection fraction
L. Rebellius, R. Berzins-Schönenberger, S. Anwer, S. Rogler, N. Kuzo, D. Schmid, A.P. Pazhenkottil, P.S. Heiniger, C. Gruner, F.C. Tanner
Department of Cardiology, University Heart Center Zurich, University Hospital Zurich, Zurich, Switzerland
Introduction: Left ventricular non-compaction (LVNC) is a rare cardiomyopathy with a progressive clinical course, resulting in symptoms such as heart failure, cardiac arrhythmias, or thrombo-embolic events. Little is known about the natural course of disease, in particular in individuals with normal LV ejection fraction (EF) at diagnosis. In this study, we aim to evaluate the outcome of this group of patients.
Methods: 48 LVNC patients with normal LV EF at diagnosis (defined as ≥50% by Simpson) were retrospectively analysed followed-up for median duration of 3656 days (2017-4965). All outcome data and conventional echocardiographic parameters were obtained; and in 27 patients, LV and right ventricular (RV) global longitudinal strain (GLS) was also determined (TomTec Image Arena).
Results: Mean age was 25.5 years. Median LVEF was 58.5% [IQR: 52.75 - 65.25]). The localization of non-compacted segments displayed a typical distribution with apical and inferolateral midventricular segments most frequently involved. Although LVEF was normal at baseline, median LV GLS was 16.8% (IQR: 20.0 - 14.2) and RV GLS was 18.7% (23.3 -15.6). Furthermore, only 30 patients (73.2%) had a normal diastolic function, while others showed impaired relaxation (19.5%; n = 8) or restrictive filling pattern (7.3%; n = 3). During follow-up, LVEF decreased slightly from the initial visit (59%, [53.3-65.0]) to last follow-up (56%, [53.0-61.8], p = 0.0009), and LV end-systolic and end-diastolic volumes increased (p = 0.009 and 0.001, respectively). The other echocardiographic parameters did not show any significant changes. The change in LVEF and LV volumes during follow-up was not significantly associated with outcome. Outcome results are shown in table 1.
Table
O54-1. Outcomes in LVNC patients with normal EF.
Outcome
N (%)
All-cause mortality
3 (6.3%)
Hospitalisation for Heart Failure
5 (10.4%)
Thrombo-embolic events
3 (6.3%)
Arrhythmic syncope
5 (10.4%)
Non-sustained ventricular tachycardia
3 (6.3%)
Other complications
9 (18.8%)
Conclusions: Patients presenting with a LVNC phenotype and normal LVEF did not display a completely normal LV function as revealed by LV strain and LV diastolic function. LVEF decreased slightly during follow-up, but was surprisingly stable in most patients. Nevertheless, a significant number of individuals experienced a clinically relevant event. Hence, a LVNC phenotype is important even in individuals with normal LVEF and such patients should be followed-up regularly.
O55
Dose adaptation of β-blockers after acute myocardial infarction
C. Bruggmann1,2, S. Fournier3, O. Muller3, F. Sadeghipour1,2, P. Voirol1,2
1Service de Pharmacie, Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne, 2Ecole de Pharmacie Genève-Lausanne (EPGL), Université de Genève-Lausanne, Genève-Lausanne, 3Service de Cardiologie, Centre Hospitalier Universitaire Vaudois (CHUV)), Lausanne, Switzerland
Introduction: The European Society of Cardiology (ESC) recommends the prescription of β-blocker (BB) after ST-segment Elevation Myocardial Infarction (STEMI). The evidences for their indication depend on the presence of a left ventricular dysfunction (LVEF<40%; Class I level A of evidence) or not (LVEF≥ 40%; Class IIa level B of evidence). In clinical practice, BB should be up-titrated to a target dose as long as the patient tolerate it.
Objectives: Assess if the BB doses prescribed at hospital discharge after STEMI are up-titrated to the target dose afterwards, and if the practice is different depending on the left ventricular function (LVEF>40% vs LVEF≥ 40%).
Method: Observational monocentric study including all consecutive patients admitted for STEMI between April 2014 and April 2016 in a tertiary hospital. BB prescriptions were assessed at discharge and after one year. Doses were classified in two categories: low (<50% of the target dose) and high (≥ 50% of the target dose).
Results: Overall, 295 patients were followed up for one year. The most frequent BB prescribed was metoprolol, (n = 216 at discharge and n = 200 at one year). The median dose was 25mg per day [Interquartile range 25; 50 mg] at discharge and after one year.
Among patients with LVEF≥ 40% (n = 239), 198 (82.9%) received a BB at hospital discharge. The dose was high for 13 (6.6%) and low for 185 (93.4%) patients. From this later group, 9 (4.9%) were up-titrated to a high dose within the year after STEMI.
Among patients with LVEF<40% (n = 56), 48 (85.7%) received a BB at discharge. The dose was high for 3 of them (6.3%) and low for 45 (93.8%) patients. From this later group, 2 (4.4%) patients were up-titrated to a high dose within the year after STEMI.
The proportion of patients having been up-titrated to a high dose within the year was not significantly different between the two groups (LVEF≥40% and LVEF<40%, p = 1.0).
Discussion and Conclusion: BB are still largely prescribed after STEMI. However, the doses are mostly low and rarely up-titrated within the year. These results are more worrying for patients with a LVEF<40%, for which the dose should absolutely be up-titrated to its maximum. Given these results, it seems necessary to investigate reasons for low dose BB prescription in clinical practice.