Joint Annual Meeting 2019 of the Swiss Society of Cardiology and the Swiss Society of Cardiac Surgery
O28
Leadless dual-chamber pacing and cardiac resynchronization therapy using conductive intracardiac communication - cumulative experience from in-vivo proof-of-concept trials
L. Bereuter1,2, T. Küffer1, A. Zurbuchen3, F. Noti1, S. Baldinger1, J. Seiler1, H. Servatius1, A. Lam1,4, R. Sweda1, B. Asatryan1, L. Roten1, H. Tanner1, T. Reichlin1, A. Haeberlin1,3,4
1Department of Cardiology, Inselspital, Bern University Hospital, University of Bern, 2ARTORG Center for Biomedical Engineering, University of Bern, 3Swiss Institute for Translational and Entrepreneurial Medicine, University of Bern, Berne, Switzerland, 4Bordeaux University Hospital (CHU), Pessac, France
Introduction: Leadless pacemakers are implanted more and more often. They overcome pacing leads, the Achilles' heel of conventional pacemakers (PMs). However, today only single-chamber leadless PMs are available, while the majority of patients requires dual-chamber devices or even cardiac resynchronization therapy (CRT). Theoretically, several leadless PMs could be implanted (e.g. in the right atrium and ventricle), but they would have to coordinate their activity wirelessly to act as dual-chamber or CRT system. Conventional telemetry is not suitable for this purpose due to its high energy consumption.
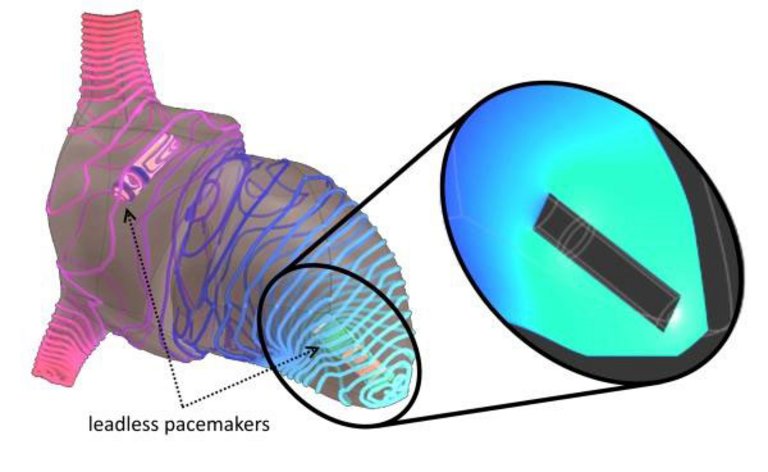
Methods: We investigated a novel method for wireless PM synchronization to build a leadless CRT system. The so-called conductive intracardiac communication uses ultra-low power alternating current (AC) signals in the order of 1 MHz, which are applied to the tissue via the PM electrodes. These AC signals propagate action potential independently with almost the speed of light through the heart and allow leadless PMs to communicate multidirectionally with each other. Computer simulations (figure O28-1) and bench tests were conducted to optimize the method. Influencing factors such as the distance between devices, myocardial hypertrophy and device encapsulation were studied. Subsequently, leadless multisite PM prototypes were developed. Leadless dual-chamber pacing and CRT implantation were performed in vivo in 5 pigs to assess safety, reliability and power consumption.
Results: The leadless PMs successfully performed dual-chamber pacing and leadless CRT in vivo. No arrhythmias were induced by the AC current and communication reliability was high (>95%). Increasing the distance between the devices negatively affects the communication (signal attenuation >10 decibel per centimeter). The figure shows the simulated attenuation of the communication signal in a heart with a ventricular PM sending out a communication message (current density isolines, arbitrary units, turquoise lines reflect higher current densities). In contrast to distance, myocardial hypertrophy and device encapsulation only have a minor impact on signal quality (attenuation <4 dB). The average transmitted power for device synchronization was <0.5 µW, corresponding to <5% of the total power consumption of contemporary leadless PMs.
Conclusions: Leadless CRT can successfully be performed in vivo using low-power conductive intracardiac communication, a promising technology for future leadless PMs.
Figure
O28-1. Simulated communication signal density distribution in a heart with two communicating leadless PMs.
O29
Stereotactic radio-ablation of refractory ventricular tachycardia: clinical outcomes
R. Jumeau1, M. Ozsahin1, J. Bourhis1, V. Vallet2, M. Zeverino2, R. Moeckli2, J. Schwitter3, M. Le Bloa4, P. Pascale4, E. Pruvot4
1Radiation Oncology, 2Radiation Physics, 3Cardiac MR center, 4Cardiology, Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne, Switzerland
Introduction: Ventricular tachycardia (VT) caused by myocardial scarring bears a significant risk of mortality and morbidity that can be partially controlled by the implantation of a cardioverter-defibrillator (ICD). Recently, stereotactic arrhythmia radio-ablation (STAR) appeared as a promising tool for the management of VT refractory to antiarrhythmic drugs (AADs) and catheter ablation (CA). We present herein the outcomes of our series of patients treated under an institutional STAR program for refractory VT.
Material and methods: Enrolled patients suffered from recurrent VT or electrical storm (ES) refractory to CA and AADs. Before the procedure, an electroanatomic mapping (EAM) was performed to localize the VT substrate (VT-sub). All patients underwent a planning CT co-registered with a cardiac MRI or a cardiac CT to help in volume definition. For each case, the cardiologist delineated the VT-sub according to the EAM data. A median dose of 25 Gy (range, 20-25 Gy) was delivered to the VT-sub.
Results: Since September 2017, five patients with VT or ES refractory to AADs and CA were treated. Four patients were elective, while another one, hospitalized in the intensive care unit (ICU), was intubated because of an ES with multiple ICD shocks refractory to CA. VT was due to an ischemic cardiomyopathy in two patients, to an inflammatory cardiomyopathy in two patients and to an idiopathic cardiomyopathy in the ICU patient. In all patients, STAR was successfully delivered using near real-time ICD lead tracking with an average time of 54 minutes. The median ablation volume was 22 cc (range, 19-35 cc). After a median follow-up of 5 months (range, 4-11), the elective patients did not experience any sustained VT recurrence or electrical shock (Panel A). The ICU patient was extubated 3 days after STAR and remained free of ICD shocks during 4 months; he presented, however, a new ES episode 19 weeks (Panel B) after the procedure related to a remote VT-sub successfully treated by CA. Importantly, after ICD interrogation, no sustained VT episodes arising from the irradiated site were detected in all patients.
Conclusion: STAR appears to be an efficient and promising tool for the treatment of refractory VT caused by myocardial scarring. Recurrence was observed only in non-ischemic cardiomyopathy at a site remote from the irradiated volume
O30
Entirely cardiac magnetic resonance-guided ventricular tachycardia substrate ablation
C. Teres1, D. Soto-Iglesias1, D. Penela2, B. Jauregui1, J. Acosta3, J. Fernandez-Armenta4, M. Linhart5, V. Syrovnev5, F. Zaraket5, R.J. Perea5, S. Prat-Gonzalez5, A. Doltra5, J.T. Ortiz-Perez5, X. Bosch5, L. Mont5, A. Alcaine6, O. Camara7, A. Berruezo1
1Heart Institute, Teknon Medical Center, Barcelona, Spain, 2Ospedale Guglielmo da Saliceto, Piacenza, Italy, 3Hospital Universitario Virgen del Rocío, Sevilla, 4Hospital Puerta del Mar, Cadiz, 5Hospital Clinic, 6Pysense, ETIC, Universitat Pompeu Fabra, 7Physense, ETIC, Universitat Pompeu Fabra, Barcelona, Spain
Background: Cardiac Magnetic Resonance-Aided VT substrate ablation using pixel signal intensity (PSI) maps from the late gadolinium enhancement-CMR (LGE-CMR) fused with the electroanatomical map (EAM) information, has shown to improve outcomes of VT substrate ablation. We sought to assess the feasibility and potential benefit of guiding the ablation procedure exclusively by CMR-derived PSI maps and heterogeneous tissue channels (HTC).
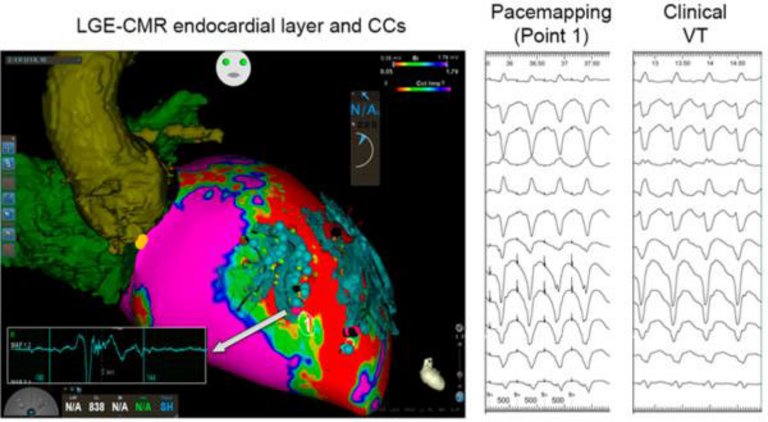
Methods: 78 patients with scar-dependent monomorphic VT who underwent substrate ablation were included. In the last 26 (33%) consecutive patients, the ablation procedure was exclusively CMR-Guided. LGE-CMR was segmented using a pixel signal intensity algorithm at 10 concentric layers from endo to epicardium. A 3D map was obtained to depict the scar core and border zone distribution. HTC were identified and segmented from LGE-CMR maps, and imported into the CARTO navigation system. Radiofrequency ablation (RFA) was delivered at all the conducting channel entrances identified on LGE-CMR. Procedural data as well as acute and follow-up outcomes were compared between the CMR-Guided and two control groups: 1) patients in whom PSI maps were available but the EAM was acquired and used to select the ablation target (CMR-Aided) 2) patients without CMR-derived PSI maps (No-CMR).
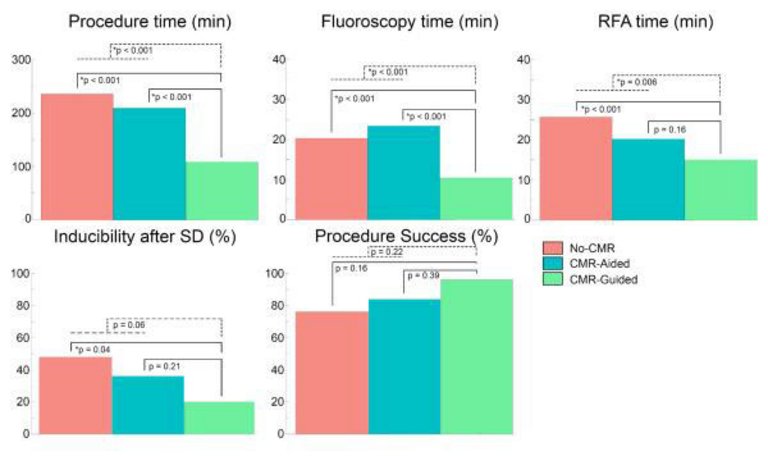
Results: Mean procedure duration was lower in CMR-Guided when compared to CMR-Aided and No-CMR substrate ablation (109±61 vs. 206±70 and 233±48 min, respectively; p<0.001 for both comparisons). CMR-Guided required less fluoroscopy time than CMR-Aided and No-CMR (11±4 vs. 23±2 and 26±11 min respectively; p<0.001 for both comparisons) and less radiofrequency (RF) time (15±8 vs. 20±15 and 26±11min; p = 0.16 and p<0.001 respectively). After substrate ablation, VT inducibility was lower in the CMR-Guided compared with CMR-Aided and No-CMR (19 vs. 35% and 46%; p = 0.21 and p = 0.04 respectively), without significant differences in end-procedure inducibility and complications. After a mean follow-up of 15,63 ± 4,06 months, there was a tendency to lower recurrence rate between CMR-Guided and No-CMR groups 2/26 (8%) vs 8/26 (31%) p = 0.09; without statistically significant difference between CMR-Guided and CMR-Aided groups 2/26 (8%) vs 4/26 (16%) p = 0.767.
Conclusion: exclusively CMR-Guided VT substrate ablation is feasible and safe, significantly reducing the procedure, fluoroscopy and RF time, and is associated to a higher non-inducibility rate after substrate ablation.
Figure
O30-1. Acute results of scar dechanneling for the No-CMR (red), CMR-Aided (blue) and CMR-Guided (green).
Figure
O30-2. LGE-CMR endocardial layer and CCs. Pacemapping at channel entrance and clinical VT.
O31
Mortality and morbidity reduction after frequent PVC ablation in patients with LV systolic dysfunction
C. Teres1, D. Penela2, B. Jauregui1, D. Soto-Iglesias1, L. Aguinaga3, A. Ordoñez1, J. Fernandez-Armenta4, L. Tercedor5, J. Acosta6, A. Berruezo1
1Heart Institute, Teknon Medical Center, Barcelona, Spain, 2Ospedale Guglielmo da Saliceto, Piacenza, Italy, 3Centro de Cardiología de Tucumán, Tucumán, Argentina, 4Hospital Universitario Puerta del Mar, Cadiz, 5Hospital Universitario Virgen de Las Nieves, Granada, 6Hospital Universitario Virgen del Rocío, Sevilla, Spain
Background: Ablation of frequent premature ventricular complexes (PVC) improves left ventricular ejection fraction (LVEF) in patients with left ventricular (LV) systolic dysfunction. This multicenter study aims to evaluate the long-term hard outcomes and potential prognostic variables in this population.
Methods: Prospective multicenter study including 101 consecutive patients [56±12 years old, 62 (61%) men] with LV systolic dysfunction and frequent PVCs referred for ablation and followed up for a minimum of 24 months. The last evaluation performed was considered the long-term follow-up (LTFUP) evaluation.
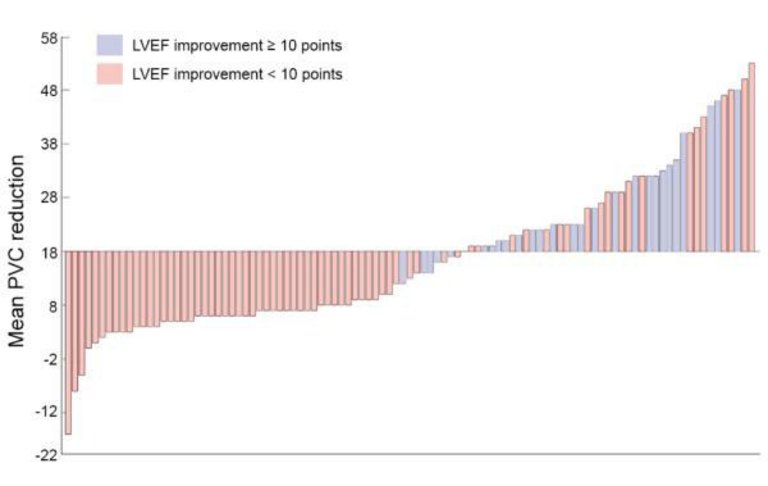
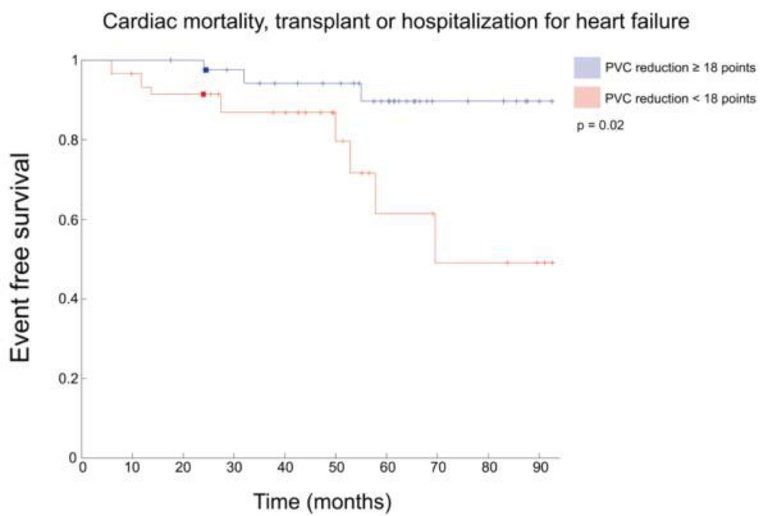
Results: Mean follow-up was 34±16 months (range 24-84 months). There was a significant reduction in PVC burden from 21±12% at baseline to 3.8±6% at LTFUP, p<0.001. LVEF improved from 32±8% at baseline to 39±12% at LTFUP (p<0.001) and NYHA class from 2.2±0.6% to 1.3±0.6% (p<0.001). BNP levels decreased from 136 [78-321] pg/mL to 68 [32-144] pg/mL (p = 0.007). Persistent abolition of >18 points of the baseline PVC burden acurately predicted a LVEF improvement of at least 10 points (Figure O31-1A) and was independently and inversely associated with the probability of cardiac mortality or cardiac transplantation [HR 0.02 (0.001-0.34), p = 0.006] as well as with the composite endpoint of cardiac mortality, cardiac transplantation or hospitalization for heart failure during the follow-up [HR 0.11 (0.25-0.46), p = 0.003], Figure O31-1B.
Conclusions: Ablation of frequent PVCs induces significant improvement in functional, structural and neurohormonal status in patients with LV systolic dysfunction, which is maintained at long term. Persistent abolition of the baseline PVC burden was associated with a reduction in the combined endpoint of cardiac mortality or cardiac transplantation.
Figure
O31-1. Waterfall plot of mean PVC reduction after ablation for predicting 10 point LVEF improvement.
Figure
O31-2. Kaplan-Meier curve combined endpoint: cardiac mortality, cardiac transplantation or hospitalization.
O32
PVC ablation in patients with prior myocardial infarction and LV dysfunction: site of origin distribution, scar burden and 1-year outcome
C. Teres1, D. Penela2, B. Jauregui1, D. Soto-Iglesias1, A. Ordoñez1, L. Aguinaga3, J. Fernandez-Armenta4, L. Tercedor5, J. Acosta6, A. Berruezo1
1Heart Institute, Teknon Medical Center, Barcelona, Spain, 2Ospedale Guglielmo da Saliceto, Piacenza, Italy, 3Centro de Cardiología de Tucumán, Tucumán, Argentina, 4Hospital Puerta del Mar, Cadiz, 5Hospital Universitario Virgen de las Nieves, Granada, 6Hospital Universitario Virgen del Rocío, Sevilla, Spain
Background: Frequent premature ventricular complexes (PVCs) can induce or worsen left ventricular (LV) systolic dysfunction. Outcomes of frequent PVC ablation in patients with LV systolic dysfunction and a prior myocardial infarction have not been described in deep.
Objective: To evaluate the outcomes of frequent PVC ablation in patients with prior MI and to characterize PVC site of origin and scar burden in this population.
Methods: Prospective multicenter study that included 54 consecutive patients [62±10 years old, 49 (90%) men, mean PVC burden 28±12%] with a previous MI [25 (46%) with an anterior MI], LV dysfunction (LVEF 34±8%) and frequent PVCs that were referred for ablation. Cardiac magnetic resonance (CMR) was performed in a subgroup of 23 (42%) patients. Scar size and characteristics were compared with a control group (n = 23) of post-MI patients without PVCs, matched by LVEF.
Results: Acute successful ablation was achieved in 47/54 (87%) patients. In 49/54 (90%) of patients, PCVs originated in the LV; the most frequent site of origin being the myocardial scar (18/54, 33,5%), followed by the LV outflow tract (LVOT) (16/54, 29%). At 1-year follow-up, PVC burden decreased from 28±12% to 4±6,8% (p<0.001); LVEF progressively improved from 34±8% to 43±11% (p<0.001)(Fig. O32-1); and NYHA class improved from 2.11±0.6 points to 1.3±0.4 (p<0.001), as compared to baseline. In the subgroup of patients studied with CMR the mean scar mass was significantly smaller than in the control group [scar mass 12±12 vs. 28±13 g (p = 0.001)(Fig. O32-2); core 5±6 vs. 13±7 g (p<0.001) and border zone 7±7vs14±7 g (0.007)].
Conclusion: PVC ablation significantly improves LVEF and functional status in patients with a prior MI. Most of the PVCs arise from the LV but only in 1/3 of the cases they originate from the MI scar; the LVOT being a frequent site of origin in this population. Furthermore, scar burden is less than half in post-MI patients with frequent PVCs as compared to those matched for LVEF without PVCs. These findings support the detrimental effect of frequent PVCs on LV function in post-MI patients and warrant an earlier indication for ablation in this group of patients.
Figure
O32-1. Mean LVEF at baseline and 12 months in patients with MI referred for PVC ablation.
Figure
O32-2. Mean scar mass in post-MI patients with and without PVCs matched for LVEF.
O33
The potential use of the His paced to RV sensed interval in optimising battery longevity in His pacing
N. Starr, G. Domenichini, C. Stettler, H. Burri
HUG, Geneva, Switzerland
Introduction: With growing evidence of long-term benefits compared to traditional right ventricular (RV) pacing, His bundle pacing (HBP) is being increasingly adopted. For safety an RV lead is often implanted to ensure ventricular pacing in case of loss of capture of the His lead. As current devices are not designed for HBP, RV pacing is usually delivered even if there is capture of the His lead, contributing to unnecessary battery decline.
In this study we evaluated the delay between pacing from the His lead and sensing from the RV channel (HP-RVS) to propose timing intervals that could avoid unnecessary RV pacing.
Methods: We studied 38 patients with HBP and a backup RV lead in which the His lead was connected to the RA port (n = 20) or to the LV port (n = 18). His threshold tests were performed with simultaneous 12 lead ECG recordings to determine selective (SHC) or non-selective (NSHC) His capture. The HP-RVS interval was measured using digital calipers. In patients with the His lead connected to the atrial port, crosstalk was also evaluated using "worst case" settings in which pacing outputs were increased to maximum allowed (8V) on the His lead alongside the lowest permissible sensitivity on the RV lead.
Results: The overall HP-RVS interval was 80ms +/- 21.4ms (range 40 to 140ms). The HP-RVS interval was shortest in cases of NSHC (73.1ms +/- 16.9ms, range 40 to 110ms) and longest in patients with SHC and uncorrected right bundle branch block (107.5 +/-23.8ms, range 70 to 140ms). Of note for each patient with the His lead connected to the atrial port there were no instances of crosstalk found.
In patients with the His lead on the LV port in which it was not necessary to correct a His paced bundle branch block through fusion pacing, the VV interval was increased to the maximum programmable value for Medtronic devices of 80ms in an effort to avoid unnecessary RV pacing. Despite these efforts to avoid RV pacing whilst maintaining it as a safety backup, it led to biventricular pacing in each patient thereby resulting in unnecessary RV pacing.
Conclusion: HP-RVS delays are shortest with NSHC and longest with SHC in cases of uncorrected right bundle branch block. Shortening the ventricular safety pacing window to 40ms and lengthening the programmable interventricular delay to 140ms could avoid unnecessary backup ventricular pacing, thereby prolonging device longevity whilst ensuring patient safety.
O34
The effects of pacing polarity on his capture thresholds
N. Starr, G. Domenichini, C. Stettler, H. Burri
HUG, Geneva, Switzerland
Introduction: Although His bundle pacing (HBP) is believed to be a more physiological form of pacing compared to right ventricular (RV) pacing, there is a paucity of data regarding the effect of polarity on His thresholds. As capture thresholds may be higher with HBP, it is important to evaluate ways to ensure a safety margin whilst increasing battery longevity, therefore we investigated the effect of pacing polarity on capture thresholds.
Methods: A threshold test was completed on 41 patients with His leads in various configurations (His on Atrial (A) (n = 19), left ventricular (LV) (n = 18) and RV port (n = 4)). Threshold tests were completed in the available polarities according to device and port type; starting at 8V at 0.4ms and 1ms, alongside a 12 lead ECG to identify the types of His activation (selective his capture (SHC) vs non-selective his capture (NSHC)) and their corresponding thresholds.
Results: When comparing bipolar versus unipolar thresholds for His capture (NSHC and SHC), there was a significant reduction in capture thresholds in unipolar compared to bipolar at both 0.4ms and 1ms (mean bipolar threshold at 0.4ms = 2.76V+/-2.06 vs 2.11V+/-1.5 in unipolar, p = 0.01E-3 whilst the mean bipolar threshold at 1ms = 2.23V+/-1.9 vs 1.77V+/-1.5 in unipolar, p = 0.03E-5, with a mean impedance in bipolar of 470Ω+/-91 compared to a lower mean impedance in unipolar of 318Ω+/-46) in the overall group. However, there was no significant difference between thresholds in extended bipolar (EB) and unipolar configurations (mean threshold in EB at 0.4ms = 2.27V+/-1.8 vs 2.04V+/-1.95 in unipolar, p = 0.275, and mean threshold in EB at 1ms = 1.6V+/-1.3 vs 1.57V+/-1.46 in unipolar, p = 0.45, with a mean impedance in EB of 400Ω +/-98 and 311.7Ω +/- 60.4 in unipolar).
In addition, we observed anodal capture at high outputs in an EB configuration in 4/18 patients (22%) when the His lead was attached to the LV port. Anodal capture occurred at high voltage outputs with an average value of 5.4V+/-2.2 at 0.4ms and 4.6V+/-0.9 at 1ms.
Conclusion: Whilst unipolar and extended bipolar pacing configurations yield significantly lower capture thresholds compared to bipolar pacing, a visible pacing spike also allows the identification of a paced rhythm with SHC. A finding we describe for the first time with HBP was an additional transition in QRS morphology during threshold tests attributed to anodal capture in the EB configuration when the His lead was connected to the LV port.
Table
O34-1. A comparison of extended bipolar (EB) and unipolar thresholds and impedances at 1ms & 0.4ms.
Total number
Pulse width (ms)
Mean EB Impedance (Ω)
Mean Unipolar Impedance (Ω)
Mean EB threshold (V)
Mean Unipolar threshold (V)
Difference in thresholds (p-value)
17
0.4
400+/-98
311.7+/-60.4
2.27+/-1.8
2.04+/-1.95
0.275
17
1
390+/-101
311.7+/- 60
1.6+/-1.3
1.57+/-1.46
0.45
Table
O34-2. A comparison of bipolar and unipolar thresholds and impedances at 1ms & 0.4ms.
Total Number
Pulse width (MS)
Mean Bipolar Impedance (Ω)
Mean Unipolar Impedance (Ω)
Mean Bipolar threshold (V)
Mean Unipolar threshold (V)
Difference between thresholds (p-value)
32
0.4
470+/-91.2
318.5+/-46.4
2.7+/-2.06
2.11+/-1.55
0.01E-3
42
1
467+/-89
318+/-45
2.2+/-1.9
1.77+/-1.5
0.03E-5
O35
Gender differences in left atrial scar burden after pulmonary vein isolation with significant impact on pulmonary vein reconnections
A. Lam1,2, F. Bourier2, K. Vlachos2, M. Takigawa2, W. Escande2, C. Andre2, R. Chauvel2, L.-J. Zeng2, J. Duchateau2, T. Pambrun2, F. Sacher2, N. Derval2, A. Denis2, M. Hocini2, M. Haissaguerre2, P. Jais2, H. Cochet2
1Department of Cardiology, Inselspital, Bern University Hospital, University of Bern, Berne, Switzerland, 2Electrophysiology and Ablation Unit, Bordeaux University Hospital (CHU), Pessac-Bordeaux, France
Introduction: Pulmonary vein (PV) isolation is an established technique for the treatment of atrial fibrillation (AF). However, the success rate is still suboptimal and varies among individuals, with especially higher recurrence rate reported in female.
The aim of the study is to assess the impact of radiofrequency (RF) on the left atrial (LA) tissue and the rate and burden of electrical PV reconnection according to gender after a first ablation for paroxysmal AF.
Method: 49 patients (12 female, 61±9y) referred to our centre for a first catheter ablation procedure for paroxysmal AF were included. All underwent cardiac magnetic resonance (CMR) at baseline to quantify LA fibrosis, and then a conventional catheter ablation procedure aiming at PV isolation. All patients underwent a follow-up CMR at 3 months to assess scar burden, followed by a systematic redo EP study, regardless of arrhythmia recurrence. During the redo EP study, the presence and burden of PV reconnection was assessed on a 16-segment model (4 segment per vein: anterior, superior, posterior, inferior). Post-ablation scar and PV reconnection characteristics were compared between male and female.
Results: All 4 PVs were successfully isolated in all patients, with no difference in RF duration between genders (P = 0.34). On the follow-up CMR, the total scar burden on PVs was significant smaller in women as compared to men (7.6±2.2ml vs 11±2.2ml, p<0.001), while the LA volume was similar (18±2.7ml vs 20±4.8ml, p = 0.274). On the follow-up EP study, female had a higher number of PV segments showing electrical reconnection (median 4.5 [IQR 2-7] vs 3 [1-4], p = 0.05), especially in the anterior RIPV (reconnected in 42% of female vs 13% male, p = 0.028) and inferior RIPV (reconnected in 83% of female vs 15% male, p<0.001) (Figure O35-1).
Conclusion: Female with paroxysmal AF show lower scar burden and higher degree of PV reconnection after PVI than male. This may explain the higher recurrence rate reported in female after catheter ablation for paroxysmal AF.
Figure
O35-1.
O36
Differences in acute and long-term block after cavo-tricuspid isthmus ablation as a stand-alone procedure versus at the end of an atrial fibrillation ablation: technical and or human factors?
B. Asatryan, A. Haeberlin, H. Servatius, J. Seiler, F. Noti, S.H. Baldinger, R. Sweda, A. Lam, N. Nozica, L. Roten, T. Reichlin, H. Tanner
Department of Cardiology, Inselspital, Bern University Hospital, Berne, Switzerland
Introduction: Bidirectional block of the cavo-tricuspid isthmus (CTI) is a well established endpoint after ablation of typical atrial flutter and clinical recurrence rate after CTI ablation is low. However, reports on long-term persistent CTI conduction block using invasive measures in different procedural settings are sparse. We aimed to investigate the acute and long-term rate of CTI conduction block as a stand-alone procedure (CTI only) versus combined with an atrial fibrillation ablation (AF plus CTI). Moreover, we compared the type of ablation catheters used with respect to acute and chronic CTI block.
Methods: All patients with CTI only and AF plus CTI procedures were included from our local AF ablation registry if they had a redo procedure with invasive assessment of CTI block (most often an AF ablation after an initial CTI only ablation or a Redo-AF ablation after an initial AF plus CTI ablation). The persistence of bidirectional CTI conduction block was tested using standard pacing manoeuvres in all patients. A comparison of acute and longterm conduction block was performed in both groups as well as a comparison of the ablation catheter used (8mm non-irrigated tip versus irrigated tip).
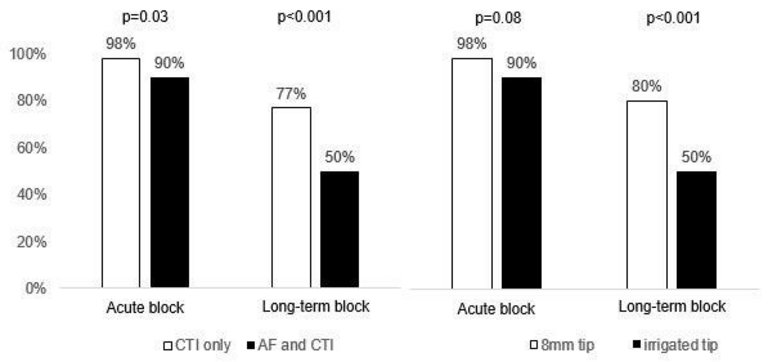
Results: In total, 198 patients were included. CTI only ablation was performed in 110 patients and AF plus CTI ablation in 88 patients. An 8mm tip catheter was used in 74% of all CTI only procedures, and an irrigated tip catheter in 91% of AF plus CTI procedures. Follow-up procedures with assessment of CTI block were done after a median follow-up of 18 months in CTI only patients, and after 10 months in AF plus CTI patients. Both acute and long-term CTI block was achieved significantly more often in the CTI only group compared to AF plus CTI group (98% vs. 90% (p = 0.03) and 77% vs. 50% (p<0.001), figure left side). Similar results were found for the comparison of 8mm versus irrigated tip catheters (figure right side).
Conclusions: Bidirectional CTI block is acutely achieved in most patients in both CTI only and AF plus CTI group. However, the percentage of long-term CTI conduction block was significantly higher in the CTI only group. A combination of human factors (exhaustion of the patient and/or the interventional staff members at the end of the AF procedure) and technical factors (higher success rate with the 8mm non-irrigated tip ablation catheter) are likely to explain the difference and both deserve further consideration.
Figure
O36-1. Acute and long-term CTI block in CTI only vs. AF and CTI and 8mm tip vs. irrigated tip.
O37
Adequate ICD treatments after the use of the wearable cardioverter-defibrillator - first results from the Swiss nationwide WCD registry
B. Kovacs1, H. Burri2, L. Haegeli3, S. Reek4, N. Krasniqi5, U. Eriksson5, F. Duru1
1Cardiology, University Hospital Zürich, Zurich, 2Cardiology, University Hospital of Geneva, Geneva, 3Cardiology, Regional Hospital of Aarau, 4Cardiology, Hirslanden Clinic Aarau, Aarau, 5Cardiology, GZO Regional Health Center, Wetzikon, Switzerland
Introduction: The wearable cardioverter-defibrillator (WCD) offers an efficacious temporary protection from arrhythmogenic death when an implantable cardioverter-defibrillator (ICD) cannot (yet) be used. The role of WCD and the patients most likely to benefit from it remains up to debate. Little is known about the rate of device implantation as well as the incidence of adequate treatments after WCD use.
Purpose: This is the first study reporting on the indications and outcomes of the use of the WCD in Switzerland focusing on device implantation rate and following treatments.Methods: We retrospectively reviewed the indications and outcomes at four medical centers prescribing WCDs over the past four years in Switzerland. Data on therapy adherence, outcomes and number of therapies by WCD and (if implanted) ICD are reported.
Results: 262 patients were included in our study. The mean age was 58 ±13years, 15% were female. Indications of WCD use were reduced ejection fraction due to ischemic cardiomyopathy (ICM) (45%), non-ischemic cardiomyopathy (NICM) (28%), inherited/congenital heart disease (0.4%), documented or suspected ventricular arrhythmia without the indication for ICD (6 and 5%, respectively), bridge to either device implantation (7%) or heart transplantation (0.8%), or other (7.8%). The median wear-time was 22.6 hours per day (interquartile range [IQR] 19.8 to 23.2 hours per day) over a median of 60 days (IQR 35-93). The number of adequate treatment by the WCD was only three (1%) while no inadequate treatments occurred. 45% of patients were implanted with an ICD. During a median follow-up of 432 days (IQR 247-708), adequate treatment occurred in 10% of implanted patients after a median of 110 days (IQR 13-256). Inadequate treatments occurred in 1.6% after a median of 378 days (IQR 201-556). Therapy by ICD was most frequent for ICM patients (50% of treated patients) as initial WCD indication.
Conclusions: ICM was the most common indication for WCD use in the Swiss cohort. Despite the rather long wear-times, the rate of adequate therapy by the WCD was low. Adequate discharges were observed in 10% of ICD recipients after several months, which may question the routine use of in the early phase of ICM.
O38
Efficacy and safety of atrial ablation procedures in patients with complete d-TGA and atrial switch at a Swiss tertiary care center
L. Roten1, N. Nozica1, E. Elchinova1, B. Asatryan1, R. Sweda1, T. Kueffer1, F. Noti1, S.H. Baldinger1, A. Lam1, A. Haeberlin1, H. Servatius1, J. Seiler1, F. Schwitz1, H. Tanner1, K. Wustmann1, E. Delacrétaz2, M. Schwerzmann1, T. Reichlin1
1Department of Cardiology, Inselspital, Bern University Hospital, University of Bern, Berne, 2Department of Cardiology, Hirslanden Clinique Cecil, Lausanne, Switzerland
Introduction: Patients with complete transposition of the great arteries (d-TGA) and atrial switch face a high lifetime risk of arrhythmias. Interventions in these patients are challenging because of their particular anatomy. Reports on ablation procedures in this patient population are scarce and missing for Switzerland.
Method: We retrospectively analyzed all ablation procedures performed in the above-mentioned population at a Swiss tertiary care center.
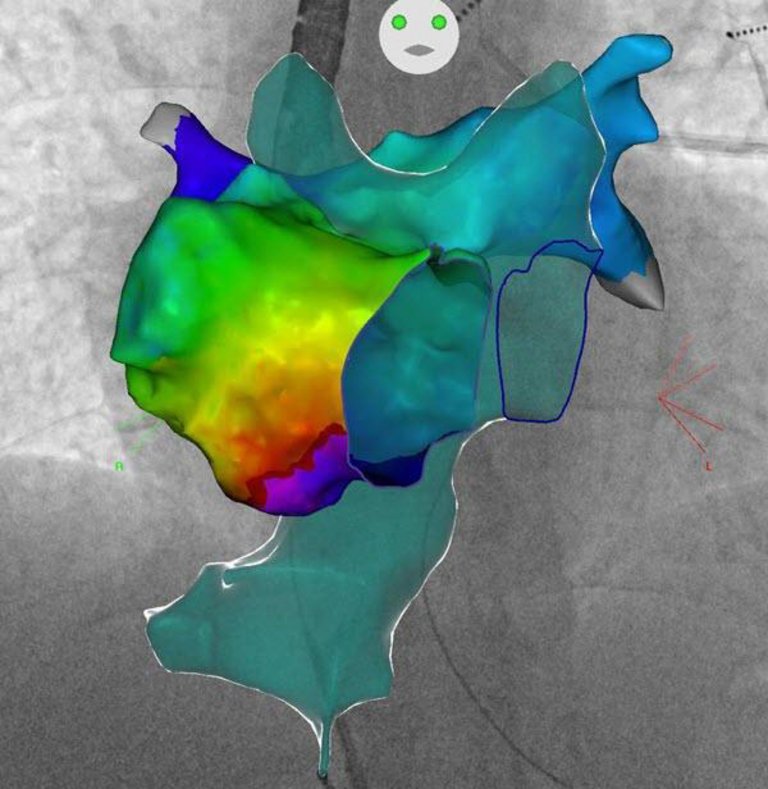
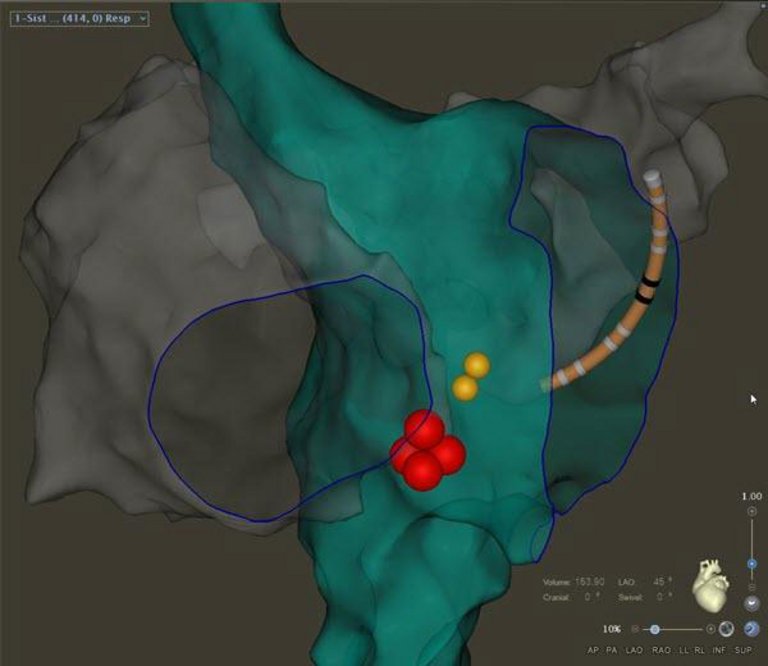
Results: Among 73 d-TGA pts. (71% male; N = 37 Senning; N = 36 Mustard) followed at our center, 17 ablations were performed in 11 pts. (15%; one ablation in 8 pts., two in 2 pts. and five in 1 patient). Median age at first ablation was 34 years (range 15-49 years). A total of 17 different intra-atrial reentry tachycardias (IART) and 3 AVNRT were targeted. Of the IART, 10 were cavotricuspid isthmus (CTI)-dependent (Figure O38-1) and 7 were not. In two procedures (12%) only the systemic venous (SV) baffle was accessed for ablation. In 15 procedures (88%), ablation was performed within the pulmonary venous (PV) baffle. Access to the PV baffle was retrograde via the aorta in 6 cases (35%), via a baffle leak in 3 (18%) and via baffle puncture in 6 (35%). All procedures with retrograde approach to the PV baffle or with SV baffle only ablation were performed up to January 2012 and all remaining procedures afterwards. The 3 pts. requiring repeat procedures had retrograde or SV baffle approaches initially, and one additional ablation via baffle puncture was successful. The CTI was targeted in 10 pts. (91%) and ablation finally successful in all with bidirectional block demonstrated in 8 pts. The coronary sinus was found to drain into the SV baffle in 5 pts. (46%) and useful for assessment of CTI block. The seven CTI-independent IART were scar-related micro-reentries. Ablation of all 3 AVNRTs was successful after one procedure without recurrence. Slow pathway ablation was performed in the SV baffle in two and in the PV baffle in one case (Figure O38-2). After a median follow-up of 7 months (range 2-186 months) 9 pts. are without recurrence and in 2 pts. rare self-limited arrhythmias still occur. No procedural complications occurred.
Conclusion: Arrhythmias in patients with complete d-TGA and atrial switch are mainly CTI-dependent IART or scar-related micro-reentries, and a few patients also have AVNRT. Ablation of these arrhythmias is safe and successful if PV baffle access is achieved via a baffle leak or baffle puncture.
Figure
O38-1. Activation map of CTI-dependent IART in a d-TGA patient after atrial switch.
Figure
O38-2. Example of a slow pathway ablation; yellow dots: His bundle; red dots: slow pathway.