Joint Annual Meeting 2019 of the Swiss Society of Cardiology and the Swiss Society of Cardiac Surgery
O17
Recurrent bleeding due to interaction of low-dose apixaban with amiodarone and the anticholinergic drug darifenacin in the context of renal insufficiency: the pitfalls of polypharmacy in elderly patients
M.P. Nägele1, V. Stork2, J.H. Beer1
1Internal Medicine, 2Pharmacy, Cantonal Hospital of Baden, Baden, Switzerland
Introduction: Direct oral anticoagulants (DOACs) have advanced the field of anticoagulation. Yet significant pharmacokinetic interactions can occur, in particular in elderly patients on polypharmacy and with impaired kidney function. An interaction between apixaban and the anticholinergic drug darifenacin has not yet been described in the literature.
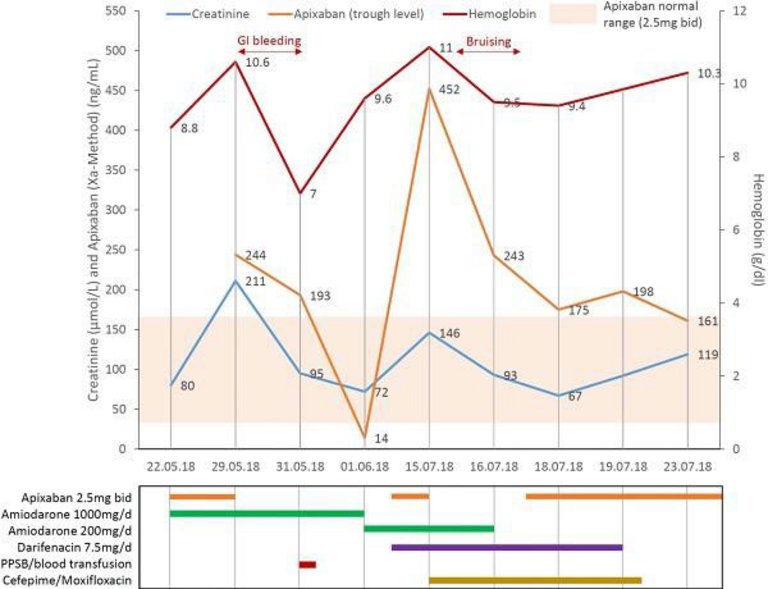
Case report: We report the case of a 93-year old female patient who presented with decompensated heart failure due to atrial fibrillation (CHA2DS2-VASc 5 points). Comorbidities included mild cognitive impairment, hypertension, osteoporosis and anemia. At admission, anticoagulation was switched from rivaroxaban 20mg daily to low-dose apixaban (2.5mg twice daily) and amiodarone was started for rhythm control along with furosemide for diuresis. Concomitant therapy included candesartan, amlodipine, bisoprolole, pantoprazole and quetiapine. In the following 6 days, she developed acute kidney injury that culminated in major upper gastrointestinal bleeding due to accumulation of apixaban (Figure O17-1). A focal bleeding site could not be identified in gastroscopy. Prothrombin complex concentrate, one red blood cell concentrate, volume and vasopressors were used for stabilization. Apixaban was paused for 2 weeks. One month later, she was readmitted for pneumonia that was treated with cefepime and moxifloxacin as well as a recurrent episode of prerenal acute kidney injury. Meanwhile, the anticholinergic drug darifenacin had been added by the general care physician for urogenital urgency. New bruising was noted, and again significant accumulation of apixaban occured. Apixaban accumulation persisted despite temporary apixaban withdrawal, cessation of amiodarone, normalization of renal function and successful antibiotic treatment. Due to its metabolism via CYP3A4 and p-glycoprotein, darifenacin was stopped as a pharmacokinetic interaction was suspected. After cessation, apixaban plasma levels normalized in the high-normal range. At follow-up, no further bleeding episodes occurred.
Conclusion: Pharmacokinetic interactions involving DOACs are common in elderly polymorbid patients, in particular with concurrent renal insufficiency and even when using lower doses. Before and during DOAC treatment, physicians should regularly check for potential interactions and adjust the dose/type of anticoagulant and potentially interacting medications accordingly to avoid complications.
Figure
O17-1.
O18
Mechanical mitral valve thrombosis in pregnancy: What now?
N. Molitor, L. Meier, T. Seeliger, D. Babic, H. Schneider, R. Hämmerli, C. Attenhofer Jost, F. Bonassin, M. Greutmann
University Heart Centre Zurich, Zurich, Switzerland
Background: In women with mechanical valves, pregnancy is considered high risk (WHO III). Because of differing maternal and fetal risks associated with various anticoagulants, the choice of optimum anticoagulant regimen remains challenging.
Case report: We report the case of a 34-year old female who underwent mechanical mitral valve replacement in 2009 due to complicated native mitral valve endocarditis. At 4 weeks of pregnancy the established high-dose (>4.5mg) Marcoumar® anticoagulation was switched to low molecular weight heparin s.c. twice daily. Peak Anti-Xa levels were measured at least weekly and dose was adjusted to maintain high therapeutic levels at a range of 0.8-1.2UI/ml.
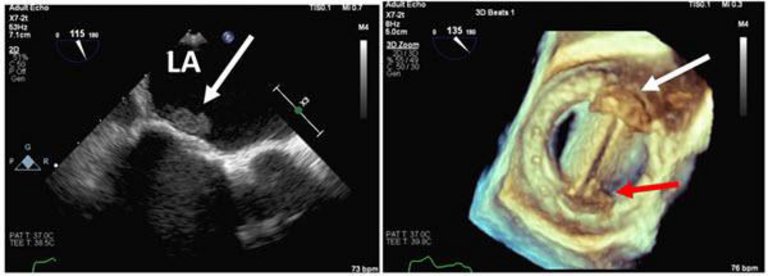
At 26 weeks pregnancy the patient complained of worsening dyspnea. Transesophageal echocardiography (TEE) revealed a large mobile prosthetic mitral valve thrombus (Figure O18-1). Marcoumar® therapy was reestablished and low dose aspirin was added. Despite change of anticoagulation, progressive thrombus mass was observed.
Decision was made to initiate a low-dose thrombolysis with t-PA according to the TROIA protocol (Özkan, Circulation 2013). TEE demonstrated almost complete resolution of valvular thrombus mass within a few hours of intravenous thrombolysis. No maternal nor fetal complications were observed and Marcoumar® therapy was restarted.
At 38 weeks pregnancy the patient underwent planned cesarean section (CS) after bridging therapy to intravenous unfractioned Heparin (UFH). Marcoumar® was reinitiated 3 days after CS. Unfortunately, 6 days post CS the patient developed massive abdominal wall hematoma (Hb 63g/l) and underwent surgical evacuation.
16 days post CS the patient suffered a large ischemic stroke with a left sensorimotor hemisyndrome, despite therapeutic UFH-therapy. Urgent intraarterial thrombectomy was successfully performed. No intracardiac thrombus was seen on TEE. Fortunately, the neurological symptoms resolved and the patient and her baby are doing fine.
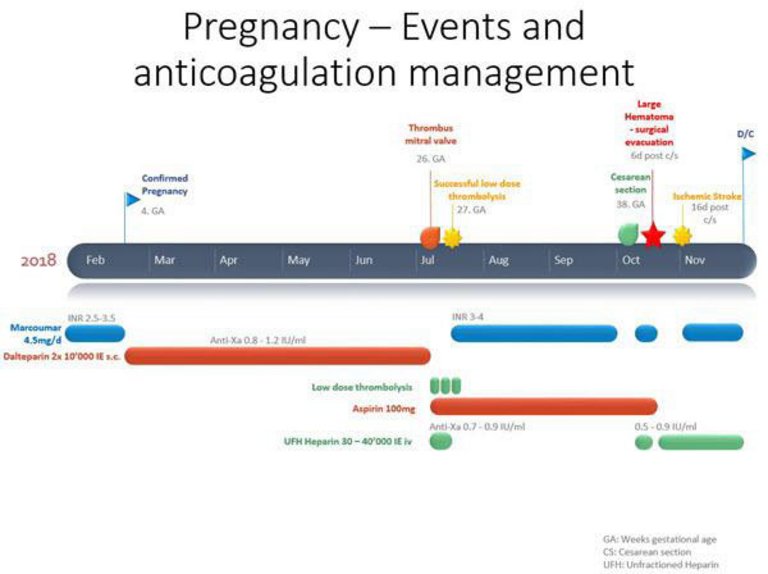
Figure O18-2 Illustrates chronological course of pregnancy.
Conclusion: Despite specialized multidisciplinary care, managing high-risk pregnancies in women with mechanical valve prostheses remains challenging. This case highlights that low-dose thrombolysis might be a safe treatment option, especially in acute mechanical heart valve thrombosis. Cesarean section offers advantages in term of logistics and anticoagulation bridging management, however higher bleeding complications after CS might outweigh this benefit.
Figure
O18-1. Transesophageal echocardiography: Thrombosis of the mechanical mitral valve (SJM 31 mm).
Figure
O18-2. Pregnancy, events and anticoagulation management.
O19
Streptococcus pneumoniae - a threat to the heart
S.A. Schlossbauer1, E. Pasotti1, L.A. Leo2, A. Caretta2, F.F. Faletra1, G.B. Pedrazzini2
A 62-year-old lady, known for diabetes mellitus typ II, presented hypotensive (100/70 mmHg) and tachycard (130/min), complaining about exertional dyspnea, cough and weight gain in the past few weeks. Oxygen saturation was reduced to 93%. Clinical examination revealed anasarca and elevated jugular venous pressure. There were fine crepitations at top of the left basal field. Laboratory findings confirmed important cardiac decompensation (NT-proBNP 13547 ng/l) and showed elevated inflammatory markers (CRP 174 mg/l, procalcitonine 2.21 ug/l, leukocytes 22.000/l, neutrophils 19.000/l). Chest-X-ray revealed important dilatation of the cardiac silhouette, strongly suspicious for relevant pericardial effusion (PE) (Figure O19-1,A). Transthoracic echocardiography (TTE) showed important, but not hemodynamically relevant PE (Figure O19-1,B+D) and severe biventricular systolic dysfunction (LVEF 15%). Blood cultures were sampled and rapidly turned positive, with important growth of streptococcus pneumoniae. Intravenous antibiotic and diuretic therapy was promptly initiated. We interpreted biventricular dysfunction and PE as secondary to pneumococcal bacteremia, after having excluded coronary artery disease by coronary angiography and autoimmune disease or chronic viral infection. Indeed, cardiac magnetic resonance confirmed, what seen in TTE, and moreover, showed pericardial thickening (Figure O19-1,C+E). During pericardial drainage 750 ml of purulent liquid were evacuated (Figure O19-2A); serological analysis was positive for pneumococcal antigen and cytological analysis showed important quantity of leucocytes (Figure O19-2B), confirming our suspicion of cardiac involvement of pneumococcal bacteremia. High-dose antibiotic therapy was continued, but as PE recurred after just a few days, we decided for pericardial fenestration. A follow-up thorax CT scan showed resolution of PE, but persistence of slight left sided pleural effusion and consolidation of the left lower pulmonary lobe (Figure O19-2C). Antibiotic therapy was therefore continued for a total of 6 weeks. The patient returned to our outpatient clinic 2 months after discharge in well-compensated cardiovascular condition. Inflammatory values had normalized. TTE showed remarkable improvement of the left ventricular systolic function (LVEF 40%).
Severe pneumoccocal infections are associated with high risk of life-threatening cardiac complications. Therefore, vaccination is pivotal in patients at risk.
Figure
O19-1.
Figure
O19-2.
O20
Giant coronary artery aneurysm associated with abdominal aortic aneurysm
S. Schukraft, J.-C. Stauffer, J.-J. Goy, G. Baeriswyl, Z. Kallinikou, S. Puricel, S. Cook, M. Togni, A. Attinger-Toller
Cardiology, Hospital and University of Fribourg, Fribourg, Switzerland
Coronary artery aneurysms (CAA) are rare with a prevalence of 0.1% to 5% in coronary angiograms. The main causes include atherosclerosis, Takayasu arteritis, congenital diseases, Kawasaki disease, infection and trauma. Observation of simultaneous CAA and abdominal aortic aneurysms (AAA) raises questions about common etiology and therapeutic strategies.
We present a case of a 78-year-old man who was admitted to our hospital with a type 5 endoleak with peri-aortic infiltration four years after successful endovascular aortic repair (EVAR) of AAA. His past medical history includes arterial hypertension and smoking. CT angiograms at time of admission revealed a rapid expansion of the AAA to 62x69 mm and a giant CAA of the right coronary artery. This CAA was measured up to 45x42 mm. (figure O20-1A). Diagnostic coronary angiogram confirmed the CAA (figure 1B/C). The CAA was included between two tight stenoses and had a good flow (wash-in and wash-out) with no evidence of parietal thrombus. The left coronary arteries were somehow ectatic. The patient underwent EVAR explant and aorto-bi-iliacal bypass grafting. Finally, the patient underwent surgical excision of the CAA with coronary artery bypass graft of the right coronary artery.
Coronary artery aneurysms, particularly of such dimensions, are rare findings on coronary angiograms. An increasing prevalence of reported concomitant CAA and AAA implies a possible common underlying etiology but a clear relationship is not established. Most CAA are asymptomatic but some patients present with effort angina or acute coronary syndrome. The primary complication is myocardial infarction, with rupture being rare. Currently, no standardized treatment protocols exist due to limited outcome data. Treatment options include surgical excision with bypass grafting, percutaneous coil embolization, covered stent insertion or conservative drug treatment (anticoagulation).
Figure
O20-1.
O21
Innovative treatment of medically uncontrolled protein-losing enteropathy after Fontan surgery: a case report
I. Ben Ali1, R. Duran2, S. Di Bernardo1, M. Prsa1, Y. Mivelaz1, S. Bressieux1, A. Weber1, S. Lava1, N. Sekarski1
1Paediatric Cardiology Unit, Woman-Mother-Child Department, Lausanne University Hospital (CHUV), 2Diagnostic and Interventional Radiology Service, Department of Medical Radiology, Lausanne University Hospital (CHUV), Lausanne, Switzerland
Background: The Fontan operation is performed as a palliative procedure to improve survival in infants born with a functionally univentricular circulation. However, there are many long-term complications of Fontan physiology. Protein-losing enteropathy (PLE) is one of the most serious complications and there is no effective therapy. We report a case of an innovative treatment of PLE in a patient with a Fontan circulation.
Case presentation: We describe the case of an 18-year-old patient with double-outlet left ventricle, common atrioventricular (AV) valve with moderate regurgitation and pulmonary stenosis. He underwent bidirectional Glenn surgery and AV valve repair without division of the main pulmonary artery at the age of 12 months. Then Due to severe AV valve regurgitation he had underwent an implantation of a mechanical valve 9 months later, followed by pacemaker implantation for postoperative complete AV block. Subsequently he underwent a fenestrated Fontan procedure using a 19-mm extracardiac conduit at the age of 7 years. Follow-up showed normal valve function and no thrombus or flow abnormality in the Fontan circulation. At the age of 11, he developed PLE. Cardiac catheterization showed mean pulmonary artery pressure of 13 mmHg without obstruction in the Fontan circuit. Following the diagnosis, a low fat diet, diuretics, sildenafil and corticosteroid were introduced, but without significant improvement of symptoms, he was admitted multiple times for albumin replacement and anticoagulation was difficult to adjust. Finally, we performed a liver lymphangiography, which demonstrated leakage of liver lymph into the duodenum through abnormal hepatoduodenal lymphatic communications. Liver lymphatic embolization was performed with ethiodized oil, which led to an increase in albumin blood level and symptom improvement.
Conclusion: PLE in patients with a Fontan circulation is a devastating condition characterized by elevated central venous pressure and profound enteric protein loss. Etiology is leakage of this albumin-rich lymph into the duodenal lumen, predominantly through focal hepatoduodenal lymphatic channels. In the case of our patient embolization of these lymphatic connections has provided at least temporary normalization of serum albumin levels and significant symptomatic improvement. Follow-up of this patient will show the long-term outcome and the potential for sustained efficacy of this procedure in the resolution of PLE.
O22
Cardiac sarcoidosis: clinical case
Q. Chatelain, A. Testuz, G. Domenichini, S. Noble, H. Burri, P. Meyer
Division of Cardiology, University Hospital of Geneva, Geneva, Switzerland
This is about a 45-year-old patient, known for an ischemic stroke in June 2017, caused by a high-risk patent foramen ovale (PFO) which was closed percutaneously in September 2017. During this hospitalization, the patient underwent thoracic CT-scan which demonstrated stage I pulmonary sarcoidosis, further confirmed by mediastinal lymphadenopathy biopsy.
During PFO closure follow-up at 6 months, the patient reported dyspnea on exertion, and the electrocardiogram (ECG) showed complete AV block.
Cardiac PET-CT showed multi-focal myocardial hypermetabolism of both ventricles consistent with active cardiac sarcoidosis. Cardiac MRI confirmed presence of significant trabeculations of the right ventricle (RV), which were enhanced after gadolinium injection. Corticosteroid therapy was rapidly started and the patient underwent tricameral pacemaker implantation.
At 3 months follow up, cardiac PET-CT showed complete normalization of metabolic uptake by both ventricles, and excluded signs of necrosis. The ECG revealed sinus rhythm, electro-driven at the level of bundle of His. Two months later, due to frequent palpitations, the patient had a 24h-Holter monitoring which showed very frequent ventricular extrasystoles (VES) (44% of total beats), as well as episodes of brief ventricular tachycardia. Cardiac PET-CT performed at this time, showed no recurrence of cardiac sarcoidosis, and cardiac MRI revealed diminished enhancement of trabeculations of the RV.
In this context, the patient was upgraded to an implantable cardioverter-defibrillator (ICD) and anti-arrhythmic treatment with mexiletine was started, allowing a significant decrease in VES (9% of total beats) on the 24h-Holter monitoring. It should be noted that multiple transthoracic echocardiographic examinations performed several times during the follow up systematically found a preserved left ventricular ejection fraction (LVEF).
This clinical case illustrates the complexity of management of cardiac sarcoidosis, particularly at the rhythmic level, and raises the question of choice between pacemaker or ICD implantation, and place of anti-arrhythmic drugs in this setting. It is also interesting to underline discrepancy between severity of ventricular rhythm disturbances and lack of metabolic activity of cardiac sarcoidosis on imagin as well as preserved ejection fraction. Finally, this clinical situation reminds us of the high prevalence of cardiac sarcoidosis in patients under 60 years of age with complete AV block.