Joint Annual Meeting 2019 of the Swiss Society of Cardiology and the Swiss Society of Cardiac Surgery
O11
A rare cause of acute coronary syndrome
B. Pitta Gros, C. Roguelov, L. Mazzolai, N. Sala, P. Tozzi
CHUV, Lausanne, Switzerland
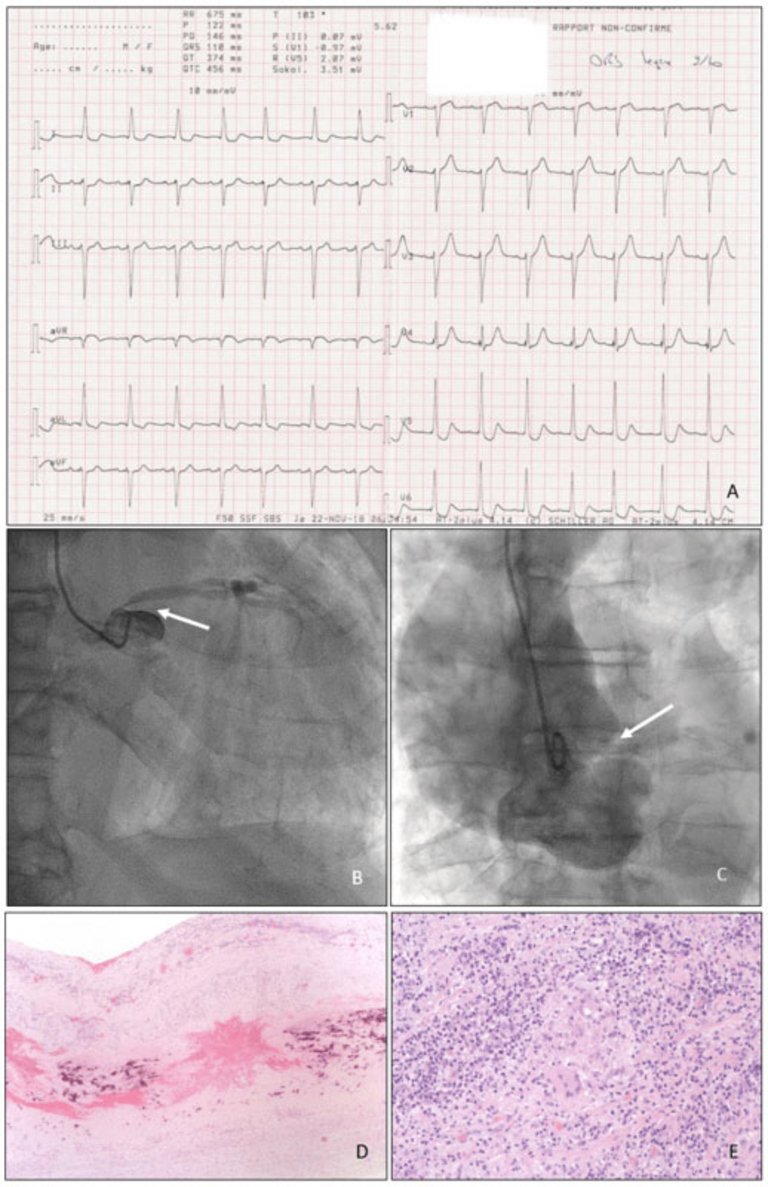
Case: A 78-year-old hypertensive man, presented to the emergency department with stabbing chest pain for two days. Physical exam showed a blood pressure of 171/96mmHg as well as a holosystolic murmur. The electrocardiogram showed ST-segment elevation in aVR combined with a ST-segment depression on the precordial leads (fig. O11-1A), cardiac enzymes were raised (troponine 876 ng/l and CK 1133 U/l). The patient was transferred for urgent angiography for acute coronary syndrome with suspected left main coronary artery (LMCA) stenosis.
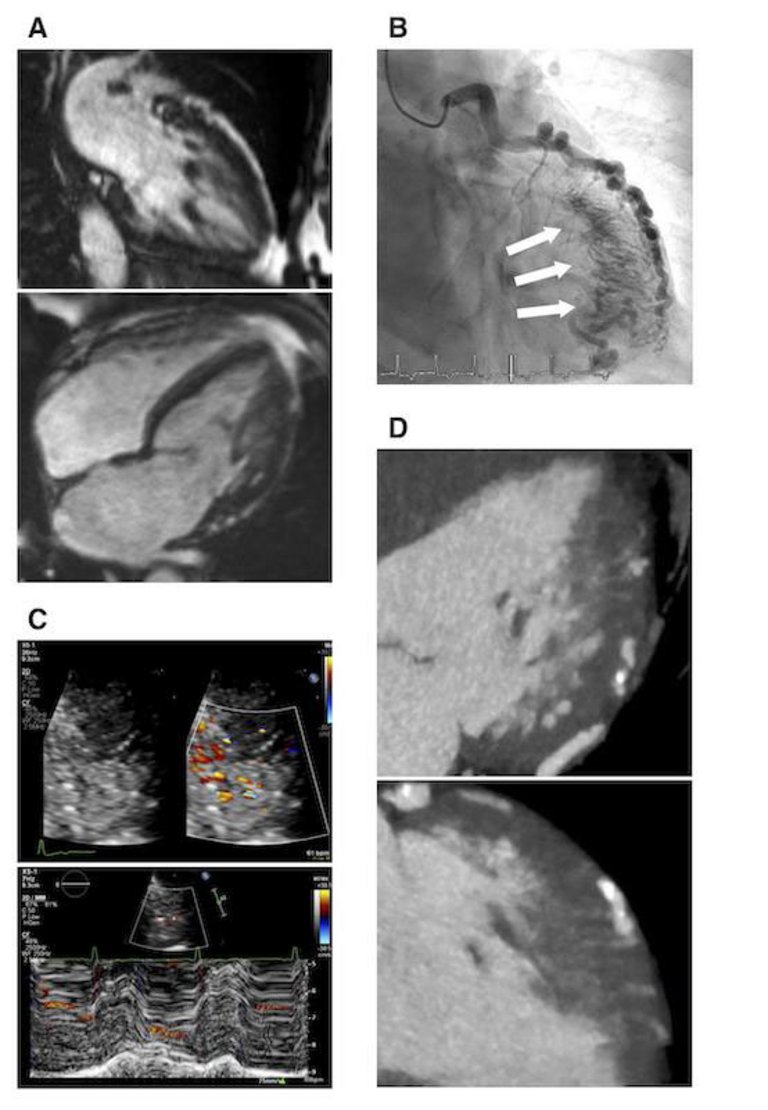
The angiography confirmed a critical stenosis of the LMCA (fig. O11-1B) but when preparing for emergency angioplasty a contrast injection revealed an aneurysm of the ascending aorta compressing the LMCA (fig. O11-1C) thus being responsible for the stenosis. The patient was taken immediately for surgery which exposed a covered rupture of the aorta with an hemopericardium for which a Bentall procedure with hemiarch replacement was performed. The patient's aorta was sent for analysis and a giant cell aortitis was diagnosed (fig. O11-1D x40 et fig. O11-1E x200). He presented no other symptoms of giant cell arteritis (GCA), a corticosteroid treatment was started and the patient evolved well afterwards.
Discussion: GCA is a systemic vasculitis that can affect large- and medium-sized arteries with an incidence of 15-33 cases per 100.000 persons aged >50 years. In patients with GCA, 20 to 40% will develop aortitis and 1 to 6% will present with aortic dissection or rupture. Patients with large artery complications often have few of the usual symptoms of GCA, causing the diagnosis to be overlooked.
Figure
O11-1. A. ECG B. LMCA stenosis C. Aortic aneurysm compressing LMCA D. Giant Cells 40x E. Giant Cells 200x.
O12
An unusual cause of Tako-Tsubo cardiomyopathy - the solution is close-by
S. Barnsteiner1, S. Sigrist2, S. Bilz2, T. Clerici3, H. Rickli4, M. Buser4
1Dept. of General Internal Medicine, 2Dept. of Endocrinology, 3Dept. of General, Abdominal, Ednocrine and Transplant Surgery, 4Dept. of Cardiology, Kantonsspital St. Gallen, St. Gallen, Switzerland
A 52 year-old woman with burning chest pain and intermittent palpitations for the past 3-4 days, unrelated to exercise or change of position, was admitted to the emergency department. Furthermore she had been suffering from an assumed viral infection of the upper airways the weeks before. Laboratory findings indicated elevated high-sensitive troponin with normal creatinine kinase levels and slightly elevated markers of inflammation. Electrocardiography showed non-significant repolarization abnormalities and a QTc of 470ms. Transthoracic echocardiography (TTE) revealed circumferential akinesia of all apical and midventricular myocardial segments with reduced ejection fraction of 40%. Coronary heart disease was ruled out by coronary CT. Cardiac MRI confirmed the echocardiographic findings of apical akinesia but did not show any late gadolinium enhancement indicative of myocarditis. The diagnosis of a possible Tako-Tsubo cardiomyopathy was proposed.
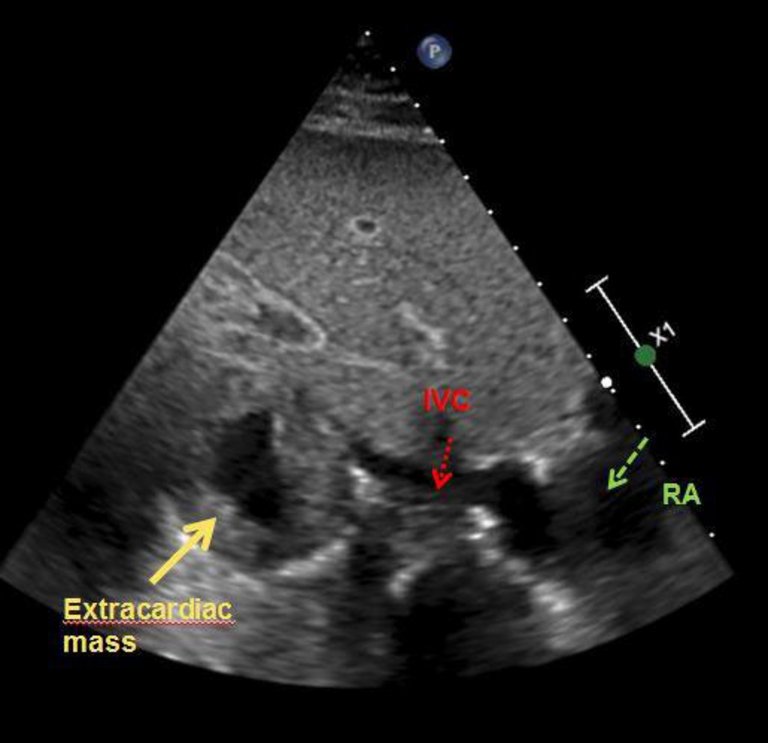
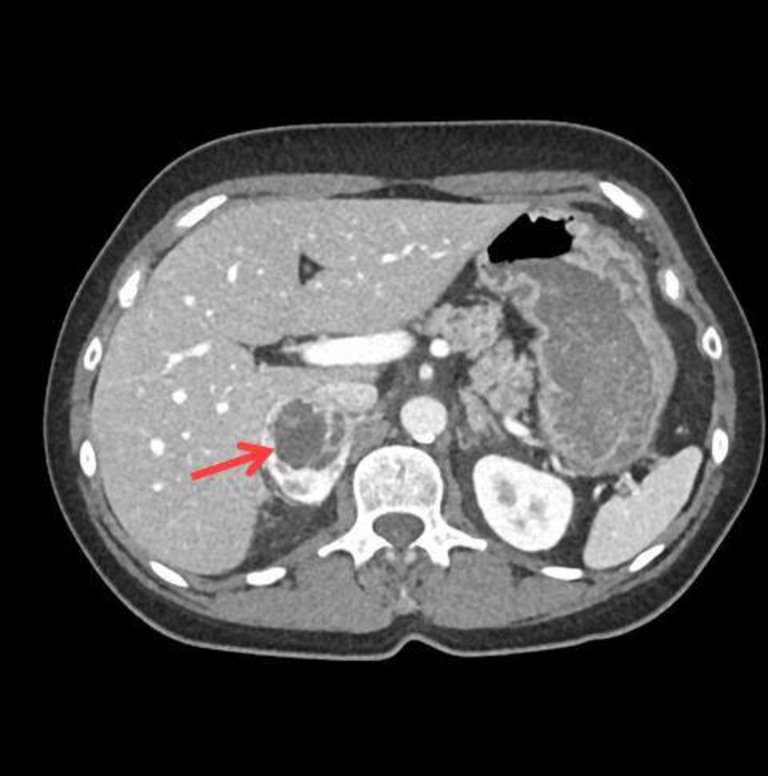
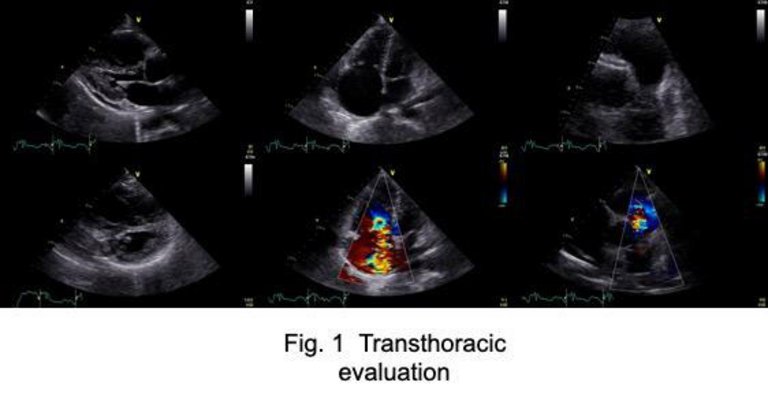
In the initial TTE a right infradiaphragmatic extracardiac mass was recognized from a substernal view (figure O12-1). In a more detailed patient history she reported paroxysmal sweats with paleness and recurrent hypertensive crises. Furthermore, a recent diagnosis of diabetes mellitus in a lean patient without family history seemed unusual. These anamnestic features and the echocardiographic finding raised suspicion of potential underlying pheochromocytoma. The diagnosis was confirmed by plasma metanephrine analysis and abdominal CT (figure O12-2). After preoperative combinationtherapy with alpha- and beta-blockers an endoscopic rightsided adrenalectomy was performed. Histologic evaluation confirmed the diagnosis without evidence for malignancy. Alpha and beta blockers were stopped on the day of surgery and since then no further antihypertensive or antidiabetic medication was needed. Ejection fraction and regional wall motion abnormalities restored within 20 days after starting initial alpha and beta blocker therapy, confirming the diagnosis of Tako-Tsubo cardiomyopathy due to pheochromocytoma.
Pheochromocytoma is a rare cause of Tako-Tsubo cardiomyopathy and can cause insulin resistance leading to hyperglycemia. Treatment leads to normalization of cardiac function and glycemic state.
In evaluating patients with suspected Tako-Tsubo cardiomyopathy potential somatic causes should be excluded before presuming a psychosocial stress factor as trigger, especially when other unclear metabolic disorders are present.
Figure
O12-1. Substernal view of TTE showing extracardiac mass projected next to the inferior vena cava.
Figure
O12-2. Abdominal contrast CT scan showing right-sided pheochromocytoma.
O13
Differing therapy responses to calcium-antagonists after surviving sudden cardiac arrest due to coronary vasospasm - a case report
D. Sepulcri1, I. Russi2,3, F. Moccetti2, S. Toggweiler2, F. Cuculi2, B. Berte2, R. Kobza2, M. Bossard2
1Department of Internal Medicine, 2Cardiology Divison, Heart Center, Luzerner Kantonsspital, Lucerne, 3Herz- und Präventionszentrum Nidwalden, Stans, Switzerland
Figure
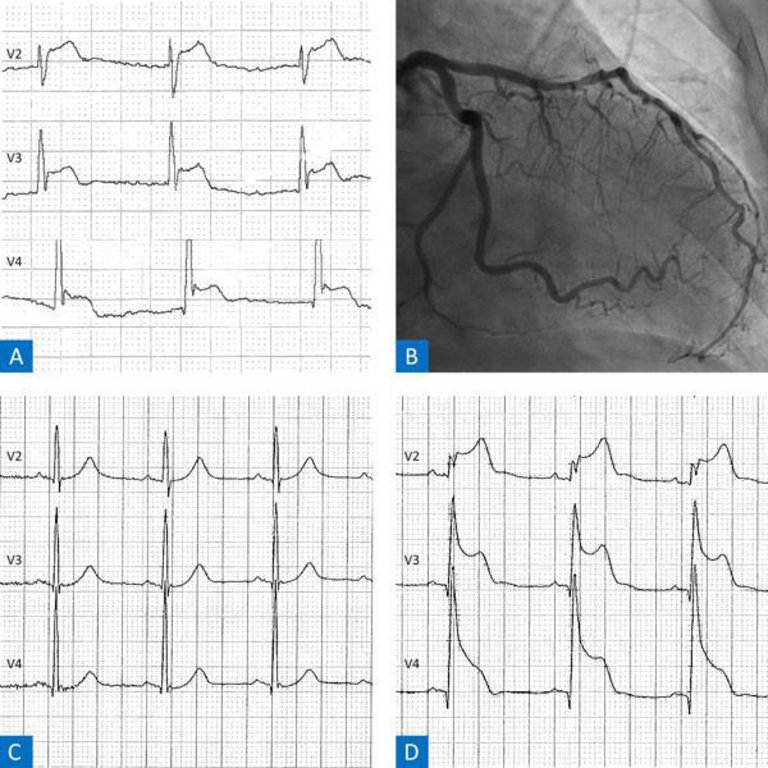
O13-1. A: Pre-hospital ECG. B: Coronary angiogram. C: ECG after ICU admission. D: Normal ECG.
Case description: A 54-year old man with known arterial hypertension was transferred to our hospital after surviving sudden cardiac arrest (SCA) secondary to ventricular fibrillation (VF) during breakfast. Cardiopulmonary resuscitation had been immediately started by his family members and continued by the emergency medical service, who defibrillated the patient three times for VF. After return of spontaneous circulation, the initial electrocardiogram (ECG) indicated sinus rhythm with ST-segment elevations in leads V2-V4 (Figure O13-1A). On arrival at our hospital, the patient was awake, and the ECG showed no abnormalities anymore. An urgent coronary angiogram was unremarkable except for mild coronary atherosclerosis (Figure O13-1B). Shortly after admission to our intensive care unit, the patient complained about chest pain accompanied by ST-segment elevations in the anterior leads (Figure O13-1C). Nitroglycerin administration promptly improved both symptoms and the ECG-changes (Figure O13-1D). Nevertheless, he developed VF, which was terminated by defibrillation. Cardiac magnetic resonance imaging was normal. Assuming Prinzmetal's angina with coronary spasm inducing severe ischemia and VF, the patient was started on verapamil. An implantable cardiac defibrillator (ICD) was implanted for secondary prevention. Subsequently the patient remained asymptomatic and was discharged after 9 days. Prior to discharge, verapamil was switched to amlodipine anticipating less drug related side effects and better long-term tolerance. While being assessed for cardiac rehabilitation, the patient reported recurrent chest discomfort at rest. A treadmill test had to be aborted due to due to angina and significant ST-segment elevations (which were responsive to nitroglycerin). Consequently, amlodipine was replaced by verapamil again and our patient remained asymptomatic ever since. The latest follow-up exam (6 months later) showed a normal treadmill test and no arrhythmias in the ICD-interrogation.
Discussion: Coronary vasospasms represent a rare cause of SCA. Besides the evaluation of an ICD, medical therapy with vasodilatators is usually suggested. While acute vasospastic attacks may respond well to nitroglycerin, calcium antagonists are the drugs of choice for long-term management. However, little is known about the effectiveness of various calcium antagonists. Our case report suggests there are relevant (pharmacological) differences, which should be considered, when managing such patients.
O14
Thebesian veins draining to the left ventricle mimicking left ventricular non-compaction
K. Durrer-Ariyakuddy, B.W. De Boeck, F. Cuculi, R. Kobza, S.F. Stämpfli
Heart Centre Lucerne, Luzerner Kantonsspital, Lucerne, Switzerland
Figure
O14-1.
Case: A 59-year old asymptomatic woman presented with lateral T-wave inversions in a routine ECG. Echocardiography suggested isolated left ventricular non-compaction (LVNC) with deep recesses and a systolic non-compacted to compacted ratio in short axis of >2. To confirm the diagnosis cardiac magnetic resonance imaging (cMRI) was performed. Quality was not optimal due to premature contractions and insufficient breath-hold, but positive diagnostic criteria for LVNC (as described by Petersen et al.) were reported (Figure O14-1A). Six years later, the patient was referred to our institution for catheter ablation of a suspected paroxysmal supraventricular tachycardia causing palpitations. Since the patient also complained about recurrent chest pain, a coronary angiogram was performed in the same session and revealed a chronic total occlusion of the right coronary artery. However, also extensive shunting from the left coronary arteries to the left ventricle through Thebesian veins (sinusoids) was observed (Figure O14-1B, arrows). In light of this new finding, echocardiography was repeated and color Doppler flow revealed diastolic filling of the recesses not from the LV cavity but from the coronary system, confirming that the irregular anatomy of the LV was not a result of incomplete LV compaction but due to the coronary anomaly (Figure 1C, apical short axis view, upper panel color Doppler in diastole, lower panel color M-mode). To exclude concurrent LVNC a cardiac CT was performed, confirming that the recesses, which initially led to the diagnosis of LVNC, exhibited diastolic flow from the coronary system (Figure O14-1C).
Conclusion: This case exemplifies that for the diagnosis of LVNC all echocardiographic criteria as defined by Jenni et al. need to be fulfilled - including color Doppler assessment of flow in the recesses. Consequently, it illustrates that cMRI alone is not sufficient for the diagnosis of LVNC but both echocardiographic and cMRI criteria need to be applied.
O15
Suspected Takotsubo syndrome relapse and asymptomatic malignant ventricular arrhythmia
E. Rigamonti, G. Vincenti, P. Antiochos, O. Muller, P. Pascale
Cardiology, University Hospital of Lausanne, Lausanne, Switzerland
Introduction: The management of pts presenting with malignant ventricular arrhythmias (VA) that have not led to syncope or aborted sudden cardiac death is challenging when the cause is considered reversible.
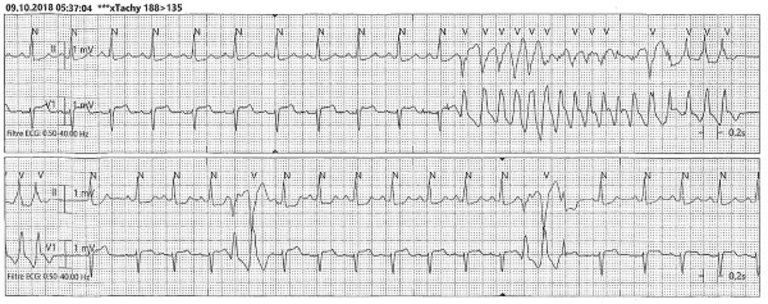
Case: A 52-yrs old widow presented to our hospital after the death of her husband because of chest pain. She had been admitted for similar symptoms 1 year before with a presumptive diagnosis of Takotsubo syndrome. A recurrence was suspected based on the emotional trigger with a typical ECG showing precordial T-waves inversion and a transient left ventricular apical ballooning at ventriculography. After the fifth night of hospitalization, the pt presented an asymptomatic unsustained polymorphic VT while awake because of a chest pain recurrence (fig. O15-1).
Such episodes had recurred almost every night and coincided with shorter salves of polymorphic VT. A chest pain recurrence was documented with 12-lead ECG. It showed a transient ST-segment elevation in the anterior precordial leads which resolved in a few minutes after the administration of nitrate (fig. O15-2).
Figure
O15-2. Dynamic ECG changes during acute chest pain.
The diagnosis of a coronary vasospasm was retained with acute ischemia acting as the VA trigger. After introduction of nitrate and calcium channel blockers, the evolution was favorable.
Considering the polymorphic VT episode, the question of implanting a prophylactic ICD was raised. We opted for an intermediate strategy consisting of a 2-month “protected” observation phase, followed by a constantly monitored follow-up. We implanted a subcutaneous loop recorder (ILR, Medtronic ® Reveal Linq) and the patient was discharged with a wearable cardioverter defibrillator (WCD, LifeVest, Zoll). After 2 months, both device did not record any VA and the WCD was removed.
Discussion: The management of coronary vasospasm associated with malignant VA remains controversial. An ICD is not recommended in case of a reversible cause but observational studies on limited cohorts have shown a high risk of recurrence. Accordingly, implantation of an ICD in addition to medical therapy is considered a class IIb indication after aborted sudden cardiac arrest in most recent guidelines. For pts at lower risk such as our pt, the value of ICD implantation is unknown. The WCD is an interesting option as it may provide protection while medical therapy and compliance are being evaluated. The constant monitoring provided by the ILR gives added security since even asymptomatic VA would be detected and would prompt ICD implantation.
O16
Severe pulmonary steno-insufficiency due to metastatic carcinoid tumor in a 57 y old patient treated by Melody Valve: first experience
V.L. Paiocchi, L.A. Leo, G.M. Viani, F.F. Faletra, G. Pedrazzini
Cardiocentro Ticino, Lugano, Switzerland
Summary: Right side heart valve involvement is a well known phenomenon in metastatic carcinoid disease. Having the most recent therapeutical progresses significantly changed the patient prognosis, bioprosthetic valves have become widely accepted for the replacement of stenotic and regurgitant native heart valves. The Melody Transcatheter Pulmonary Valve (Melody TPV, Medtronic, Minneapolis, MN, USA) has been approved for the management of failing biologic prostheses, conduits, and native valve pathology in pulmonary position. We present first case in literature of a 57-year-old woman patient with metastatic Carcinoid Syndrome with severe steno-insufficiency of pulmonary valve, symptomatic for worsening dyspnea and progressive signs of right heart failure treated with implantation of a MELODY prosthesis successfully.
Case Report: The 57-year-old woman is known since 2007 for metastatic Carcinoid Syndrome treated by surgical resection followed by chemotherapy (tamoxifene, everolimus) and radiotherapy. For 2 years she has been know for tricuspid and pulmonary involvement both of them progressing during the last years and leading to symptomatic right heart failure requiring high dosage of diuretics.She was therefore submitted to extensive imaging evaluation and to right heart catheter. Transthoracic echocardiogram (Fig. O16-1), cardiac MRI and right heart catheter confirmed severe steno-insufficiency of the pulmonary valve. The cardiopulmonary test revealed a severe limitation of aerobic exercise capacity (VO2 max 14.4 ml/min/kg
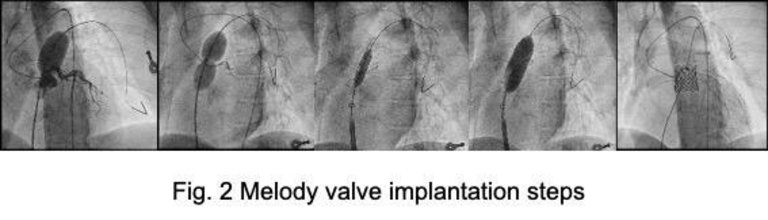
After intensive heart team discussion the decision was taken to treat the patient in a 2 step approach, initially by Melody valve of the pulmonary valve and in a second step by surgical repair of the tricuspid valve. The procedure was performed with placement of a 39x 25 mm (ANDRA) stent and subsequently a 22 mm MELODY valve was implanted successfully (Fig. O16-2). During the procedure the patient required administration of Octeotride for hypotension. The post-operative echocardiogram showed a significant reduction of the gradient on the pulmonary valve. The progressive retraction of the tricuspid valvular leaflets could not be treated with a percutaneous approach, but a surgical approach will have to be evaluated in a second step.
Conclusion: This report describes the first case in literature of severe pulmonary steno-insufficiency due to metastatic carcinoid tumor in a 57 y old patient treated by Melody Valve, successfully.