A rare entity that should be recognised by both cardiologists and radiologists to avoid misinterpretation in cardiac imaging.
A 70-year-old patient was admitted to our hospital for biological valve replacement due to aortic valve insufficiency. As cardiovascular risk factors, there was a known history of persistent atrial fibrillation, arterial hypertension, hypercholesterolaemia and suspended nicotine abuse.
At admission, he presented with stable dyspnoea of New York Heart Association grade III and increasing fatigue, but showed no signs of angina pectoris, orthopnoea or dizziness.
Preoperative laboratory analyses showed increased N-terminal pro-brain natriuretic peptide (NT-Pro-BNP), in the context of cardiac congestion. Routinely performed transthoracic echocardiography showed increased pulmonary arterial pressure and eccentric hypertrophy of the left ventricle. Ectasia of the ascending aorta was suspected. At the level of the orifice of the left atrial appendage (LAA), a thin membrane could be demonstrated with no detectable opening. However, colour Doppler showed persistent blood flow between the left atrium and the atrial appendage that was independent of systole and diastole. There was no evidence of thrombogenic material in relation to the orifice (fig. 1). As the patient had never before undergone LAA surgery, a possible idiopathic stenosis of the orifice was suspected.
Figure 1
Echocardiography with Doppler mode in modified short axis view at the level of the aortic valve. There is a thin hyperechogenic membrane at the level of the orifice of the left atrial appendage. Blood flow between the left atrium and the atrial appendage is persistent.
The LAA is a cardiac structure adjacent to the left atrium positioned to the sternocostal surface and in direct contact with the pulmonary trunk. There is wide variation in its morphological and anatomical appearance, and it has functional and structural properties different from those of the left atrium. There is still lack of scientific evidence to define a quantitative limit for a diagnosis of stenosis of the LAA.
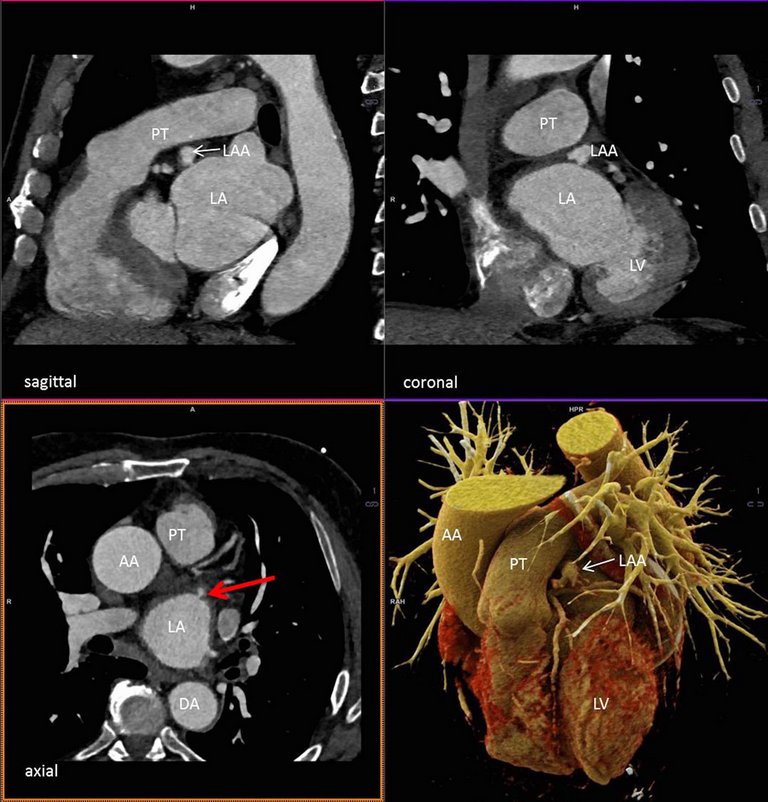
In an autopsy study, Veinot et al. [1] found a size range of the ostium of 6 to 20 mm in men and 5 to 18 mm in women. In our patient, contrast-enhanced, ECG-triggered cardiac computed tomography was performed. Ectasia of the ascending aorta could be confirmed (ca. 43 mm, fig. 2). Corresponding to the membranous structure at the orifice of the LAA on ultrasound, a narrow 3-mm opening at the orifice of the LAA could be demonstrated in multiplanar reconstructions, supporting the suspected diagnosis of a stenosis of the LAA (fig. 3). As with the echography, there was no evidence of thrombus in the LAA.
Figure 2
Computed tomography demonstrating the ectasia of the aorta in three planes (syngo.via, Siemens, with additional 3D cinematic VRT). AA = ascending aorta; DA = descending aorta; LA = left atrium; LV = left ventricle; PT = pulmonary trunk; RV = right ventricle
Figure 3
Computed tomography demonstrating the stenosis of the LAA in three planes (syngo.via, Siemens, with additional 3D cinematic VRT). AA = ascending aorta; DA = descending aorta; LA = left atrium; LAA = left atrial appendage; LV = left ventricle; PT = pulmonary trunk; RV = right ventricle
Patients with atrial fibrillation are at higher risk of thromboembolic events, with the LAA as common location of thrombus formation. There are studies suggesting that the risk for stroke and other thromboembolic events depends on the shape and morphology of the LAA [2]. Masci et al. [3] did a phantom study assessing functional parameters at the LAA orifice and suspected that not only morphology but also its geometric characteristics possibly influence the thrombogenic risk. Therefore, an idiopathic narrowing of the orifice due to a stenosis, as was suspected in our patient, could possibly imply a much higher risk for thromboembolic events. However, left atrial appendage stenosis is a rare entity and there are only few cases described in literature. Its clinical relevance remains unclear.
Following catheter angiography, our patient underwent valve replacement. Intraoperatively, the LAA was inspected and appeared very small in volume. Surgical occlusion was not performed.
There were no postoperative complications. The immediate examination was adequate. Further echocardiographic monitoring is planned. To evaluate the thromboembolic risk for the patient, the LAA will be routinely checked for thrombotic material.
Conclusion
Although the clinical significance of a stenosis of the LAA is unclear, it still may present as morphological anomaly in echocardiography that may lead to further diagnostic work-up. Computed tomography may contribute to morphological correlation with 3D datasets and high spatial resolution. This rare entity should be recognised by both cardiologists and radiologists to avoid misinterpretation in cardiac imaging.
Correspondence
Jonas Fischer, MD, Kantonsspital Baden, Im Ergel 1, CH-5404 Baden
References
1Veinot JP, Harrity PJ, Gentile F, Khandheria BK, Bailey KR, Eickholt JT, et al.Anatomy of the normal left atrial appendage: a quantitative study of age-related changes in 500 autopsy hearts: implications for echocardiographic examination. Circulation. 1997;96(9):3112–5. doi:. http://dx.doi.org/10.1161/01.CIR.96.9.3112PubMed
2Di Biase L, Santangeli P, Anselmino M, Mohanty P, Salvetti I, Gili S, et al.Does the left atrial appendage morphology correlate with the risk of stroke in patients with atrial fibrillation? Results from a multicenter study. J Am Coll Cardiol. 2012;60(6):531–8. doi:. http://dx.doi.org/10.1016/j.jacc.2012.04.032PubMed
3Masci A, Barone L, Dedè L, Fedele M, Tomasi C, Quarteroni A, et al.The Impact of Left Atrium Appendage Morphology on Stroke Risk Assessment in Atrial Fibrillation: A Computational Fluid Dynamics Study. Front Physiol. 2019;9:1938. doi:. http://dx.doi.org/10.3389/fphys.2018.01938PubMed