Gadolinium-free MR can be used for pre-procedural annular and iliofemoral assessment, and thus selection of prosthesis size.
Introduction
Transcatheter aortic valve implantation (TAVI) is now routinely performed in high-risk and intermediate-risk patients with low mortality- and complication rates. Although periprocedural risks have been substantially minimized since the introduction of TAVI, procedure- and contrast-induced acute kidney injury (AKI) remains a major concern [1, 2].
In patients undergoing TAVI evaluation, contrast media (CM) is used for multislice computer tomography (MSCT) of the chest, abdomen and pelvis, left heart catheterization, aortography, and peripheral angiography [3]. Furthermore, a significant amount of CM is additionally administered during the actual TAVI procedure [4, 5]. Among patients undergoing TAVI requiring CM-based procedures, pre-existing CKD represents one of the major predictors for AKI [4, 6–8].
We assessed the feasibility and safety of a novel integrated approach aiming to minimize periprocedural administration of CM and therefore reducing the AKI-risk in patients with severe CKD undergoing TAVI. In this context, we used gadolinium-free magnetic resonance tomography (MR), instead of MSCT for sinoannular and iliofemoral assessment and therefore valve selection. Moreover, we aimed to minimize administration of CM during coronary angiogram and TAVI in afflicted patients.
Methods
Study population
Consecutive patients undergoing TAVI for the treatment of severe symptomatic aortic stenosis between February 2016 and July 2017 were enrolled. All patients with severe CKD (glomerular filtration rate (GFR) <30 ml/min/m2) were screened and managed with our integrated approach in order to minimize administration of CM (table 1).
Table 1
Integrated approach to optimize the management of patients with severe chronic kidney disease undergoing transcatheter aortic valve replacement.
Magnet resonance tomography without gadolinium instead of multislice computed tomography
Coronary angiography with 3-4 views
Prehydration with 500 ml of saline 0.9%
Transcatheter aortic valve replacement under conscious sedation
Rapid pacing for determination of implant view
Transthoracic echocardiography to assess paravalvular regurgitation
Careful postprocedural monitoring and care
For the pre-procedural coronary angiogram and for TAVI itself, we aimed to reduce the amount of CM to a bare minimum. In addition, gadolinium-free MR was performed for annular and iliofemoral assessment, and valve sizing. Data were collected throughout the initial hospital stay and a clinical follow-up was conducted at 30 days post-procedure. The study complies with the declaration of Helsinki. Prospective data acquisition after TAVI was approved by the local ethic committee. All patients provided written informed consent.
TAVI work-up and MR protocols
Potential TAVI candidates were discussed by the interdisciplinary HeartTeam consisting of non-invasive cardiologists, interventional cardiologists, and cardiac surgeons.
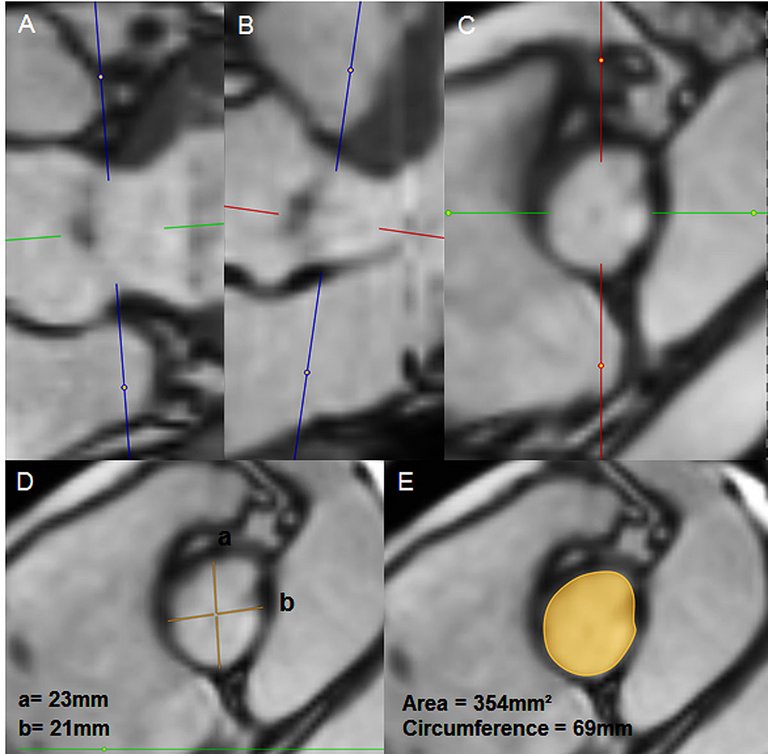
For assessment of the coronary arteries, all patients underwent a pre-procedural coronary angiogram. In patients with severe CKD, only 2-4 injections using 2-6 ml of CM were performed to visualize the left and right coronary artery. The aortic root and the iliofemoral arteries were not visualized. Instead, for annular and iliofemoral measurements, a gadolinium-free MR was performed (examples are illustrated in figures 1 and 2). MRs were performed with a 1.5 T or 3 T scanner (Siemens Magnetom Aera or Siemens Magnetom Skyra, respectively, Siemens AG, Munich, Germany). For the assessment of the aortic annulus and aortic root a non contrast-enhanced navigator-gated 3-D whole heart acquisition during the diastolic phase was conducted using fast low angle shot (FLASH) gradient-echo sequence with fat saturation and T2 preparation. The imaging parameters on the 3T scanner were as follows: repetition time/echo time 308.5/1.4 milliseconds, flip angle 20 degrees, bandwidth 610 Hz/pixel, field of view 300 × 400 mm, matrix 192 × 256, slice thickness 1.0mm, and voxel size 1.5 × 1.5 × 1.0 mm3. The imaging parameters on the 1.5 T scanner were as follows: repetition time 285.5/echo time 1.5 ms, flip angle 90 degrees, bandwidth 590 Hz/pixel, field of view 240 × 320, matrix 173 × 256, slice thickness 0.8mm, and voxel size 1.4 × 1.2 × 0.8 mm3. A total of 44 overlapping slices were acquired. Double-oblique transverse views transecting through the most caudal attachments of all three native cusps were reconstructed to measure the annular perimeter and area with a 3-D reconstruction tool allowing for free navigation and image plane selection in the 3D data set (Merlin Diagnostic Workcenter, Phönix-PACS GmbH). Distances to the right and left coronary ostium was measured perpendicular to the annulus plane. Unenhanced MR angiography using a quiescent-interval single-shot (QISS) sequence was performed to assess suitability of iliofemoral access for transfemoral TAVI approach. The optimized QISS pulse sequence used the following imaging parameters: repetition time/echo time/ invertion time/ flip angle/ bandwidth = 667.6 ms / 1.74 ms / 345 ms / 111 degrees / 660 Hz/pixel. The acquisition matrix was 260 × 400/, field of view 260 × 400/mm, slice thickness 3/mm with slices overlap 0.6/, maintaining spatial resolution at 1 mm × 1 mm × 2.4 mm3/ at 3 T and at 1.5 T, respectively. Two consecutive acquisition blocks from the infrarenal aorta to the proximal femoral arteries of overall 100 overlapping slices were acquired. Multiplanar reconstructions were derived in order to measure vessel diameters orthogonal to their longitudinal axis.
Figure 1
Gadolinium-free magnet resonance tomography for transcatheter aortic valve replacement work-up in patients with severe chronic kidney disease. Sagital (A) and coronal oblique (B) views with the corresponding double-oblique transverse view transsecting through the most caudal attachments of all three native cusps of the aortic valve (C). Measurements of the diameter (D), the area and circumference (E) of the aortic annulus.
Figure 2
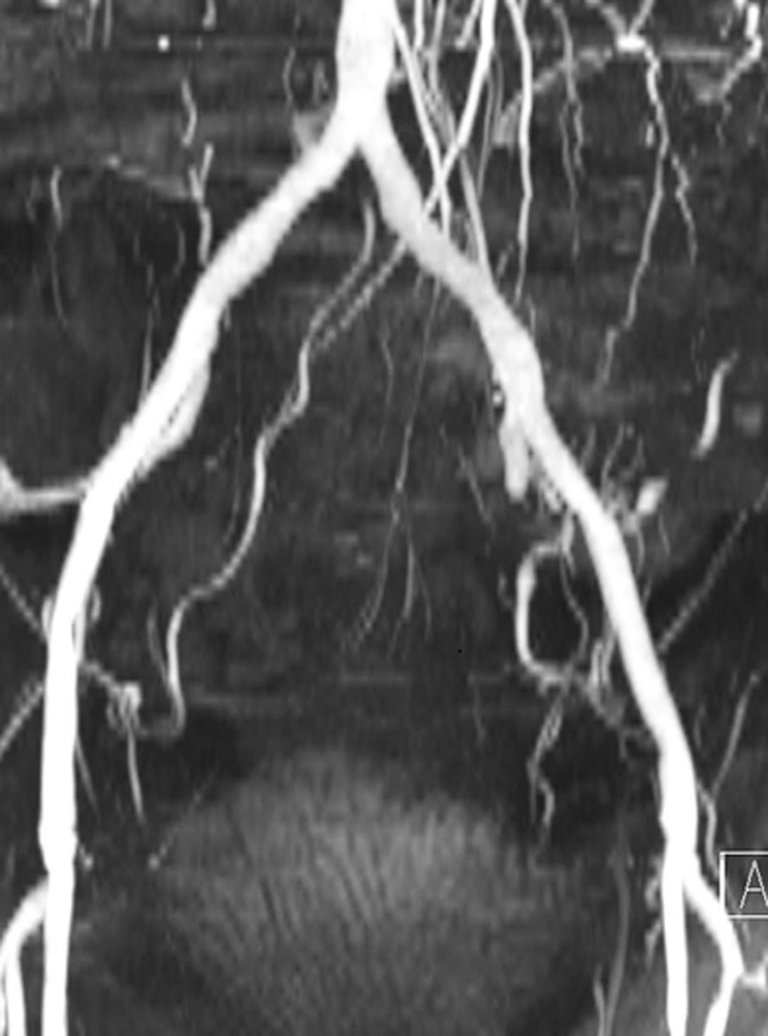
Gadolinium-free magnet resonance angiography to assess suitability of iliofemoral access for transfemoral TAVI approach.
In patients without severe CKD, TAVI work-up was performed with MSCT of chest, abdomen and pelvis using standardized protocols [9, 10].
TAVI procedure
The procedure was performed in conscious sedation in patients undergoing TAVI via the transfemoral approach and in general anesthesia for the transapical approach. We implanted the following valves: (1) ACURATE neo (Boston Scientific, Marlborough, Massachusetts), (2) SAPIEN 3 (Edwards Lifesciences, Irwine, California), (3) Evolut R (Medtronic Inc., Minneapolis, Minnesota) and (4) Allegra (NVT, Hechingen, Germany and Muri, Switzerland). Valve sizing was based on the annular perimeter (ACURATE neo, Evolut R or Allegra) or on the area (SAPIEN 3).
Procedural modifications in patients with severe chronic kidney disease
In patients with severe CKD coaxial valve implantation angle was derived from MR and reassessed with injection of contrast media prior to valve implantation. For lowering the amount of CM during implantation, rapid pacing was performed to allow full visualization of the three cusps with approximately eight ml of CM. In patients with severe CKD, paravalvular regurgitation was assessed with transthoracic echocardiography instead of a supravalvular contrast injection. Following TAVI, patients’ kidney function was closely monitored until creatinine was stable.
Definitions
Severe chronic kidney disease was defined as an estimated glomerular filtration rate (GFR) of less than 30 ml/min/m2 prior to TAVI. The estimation was performed using the Cockcroft–Gault equation. Clinical endpoints were defined according to the updated definitions of the Valve Academic Research Consortium VARC-211. Acute kidney injury was defined as an increase in serum creatinine during the first seven days after valve implantation. Stage 1 was defined as an increase in serum creatinine to 150‒200% compared with baseline or an increase in serum creatinine of 26.4 mmol/l (>0.3 mg/dl). Stage 2 was defined as an increase to 200‒299% compared with baseline. Stage 3 was defined as an increase to 300% or more compared with baseline or serum creatinine of 354 mmol/l (4.0 mg/dl) with an acute increase of at least 44 mmol/l (0.5 mg/dl). Necessity of renal replacement therapy was considered as AKI stage 3.
Statistical analysis
Categorical variables are displayed as absolute numbers and percentages, and continuous variables are presented as means (±standard deviations) or medians (interquartile ranges [IQR]), as appropriate. P-values were calculated using paired t-tests, Fisher’s exact test, χ2 test, and Wilcoxon rank-sum test, where applicable. Kaplan-Meier analyses were performed to estimate survival rates at 6 months. Statistical analyses were conducted with STATA version 13 (StataCorp, College Station, Texas, USA) and tested using 2-sided tests at a significance level of 0.05.
Results
From February 2016 to July 2017, 168 patients (55% women) with a mean age of 81±6 years were enrolled. A total of 20 patients (65% women) with severe CKD and without renal replacement therapy were treated using an integrated approach aiming to minimize contrast media. The other 148 patients (53% women) underwent standardized TAVI work-up and procedure, including MSCT. As highlighted in table 2, the baseline characteristics were balanced except for Society of Thoracic Surgeons Predicted Risk of Mortality and GFR.
Table 2
Baseline characteristics.
All patients (n = 168)
Patients with severe CKD (n = 20)
Patients without severe CKD (n = 148)
p value
Age, years
81±6
84±6
81±6
0.05
Female sex
92 (55%)
13 (65%)
79 (53%)
0.35
Hypertension
142 (85%)
17 (85%)
125 (84%)
1.0
Diabetes
30 (18%)
4 (20%)
26 (18%)
0.76
Coronary artery disease
83 (49%)
9 (45%)
74 (50%)
0.81
Prior stroke
19 (11%)
1 (5%)
18 (12%)
0.48
STS PROM, %
4.3±3.7
8.2±4.0
3.8±3.4
<0.01
Echocardiographic parameters
Aortic valve area, cm2
0.76±0.19
0.7±0.22
0.77±0.19
0.16
Mean gradient, mmHg
47±17
45±13
48±18
0.52
Left ventricular ejection fraction, %
59±13
51±15
58±13
0.03
Laboratory parameters
Creatinine (µmol/L)
107±56
198±62
94±42
<0.01
GFR ( ml/min)
54±24
24±5
58±23
<0.01
Implanted valve
Acurate neo
106 (63%)
14 (70%)
92 (62%)
0.95
Sapien 3
49 (29%)
5 (25%)
44 (30%)
Evolut R
10 (6%)
1 (5%)
9 (7%)
Allegra
3 (2%)
0 (0%)
3 (2%)
Data are displayed as n (%) or mean±SD. CKD = chronic kidney disease; GFR = glomerural filtration rate; STS PROM = Society of Thoracic Surgeons Predicted Risk of Mortality
Use of contrast media for TAVI work-up and procedure
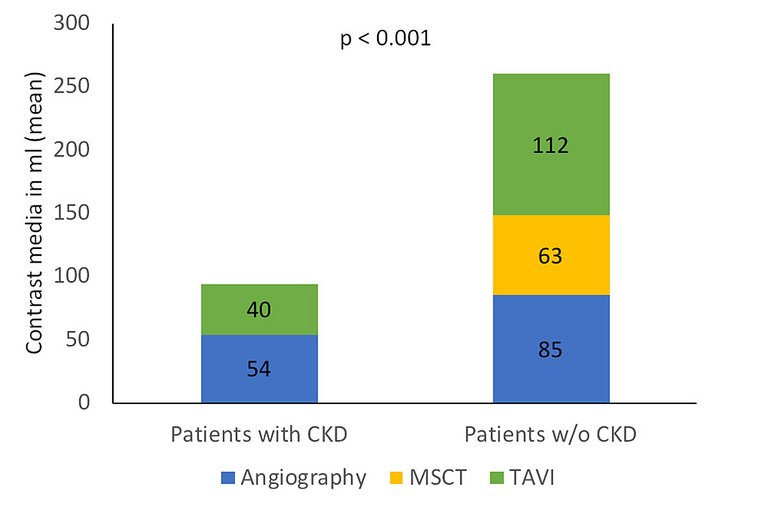
Use of contrast media is summarized in figure 3. Pre-procedural coronary angiography was performed with 54±35 ml of CM in patients with severe CKD versus with 85±44 ml in patients without severe CKD (p <0.01). Patients without severe CKD underwent ECG-gated MSCT requiring 63±14 ml of CM. TAVI was performed with 40±32 ml and 112±50 ml of contrast media, respectively (p <0.01). The total amount of CM required for pre-procedural planning and TAVI was 94±54 ml in patients with severe CKD and 260±79 ml in patients without (p <0.01).
Figure 3
Use of contrast media for TAVI work-up and procedure. Figure legend: CKD: chronic kidney disease; MSCT: multislice computer tomography; TAVI: transcatheter aortic valve replacement; w/o: without.
In-hospital outcomes
Procedural results of both groups are listed in table 3. Following TAVI, paravalvular regurgitation was none/mild in 20/20 (100%) with severe CKD and in 146/148 (99%) without (p = 0.85). AKI stage 1 was more common in patients with severe CKD (4/20, [20%] versus 9/148 [6.1%], p = 0.24). AKI stage 2 or 3 occurred in 1/20 (5%) versus 5/148 (3%) of patients with and without severe CKD, respectively (p = 0.54). One patient in each group required dialysis. Implantation of a new permanent pacemaker was required in 2/20 (10%) and 4/148 (2.7%, p = 0.15). Median duration of hospitalization was longer in patients with severe CKD than in those without (15 [interquartile range {IQR}] 5‒46) days days versus 9 days [IQR 3‒57] days, p <0.01).
Table 3
In-hospital outcomes.
All patients (n = 168)
Patients with severe CKD (n = 20)
Patients without severe CKD (n = 148)
p value
Aortic valve area, cm2
2.1±0.5
2.1±0.5
2.1±0.5
0.64
Mean gradient, mmHg
6.8±3.6
5.5±3.3
6.9±3.7
0.12
Paravalvular regurgitation
none/trace
103 (64%)
12 (60%)
91 (64%)
0.85
mild
57 (35%)
8 (40%)
49 (35%)
moderate
2 (1.2%)
0 (0%)
2 (1.4%)
Acute kidney injury stage 2 or 3
5 (3.0%)
1 (5.0%)
4 (2.7%)
0.054
CKD = chronic kidney disease
30
day and 6 month outcomes
At 30 days, there were no strokes, and survival was 20/20 (100%) among patients with severe CKD and 145/148 (98%) in those without (p = 0.68) (table 4). Major vascular complications (1/20 [5%] and 10/148 [6.8%], p = 1.0) and major or life-threatening bleeding 1/20 (5%) and 11/148 (7.4%), p = 1.0, respectively) were similar in both groups. Early safety, clinical efficacy and device success endpoints at 30 days did not differ and were high in both groups. Kaplan Meier estimates of survival at 6 months were 100% and 93.8% in patients with and without severe CKD, respectively (log rank p = 0.31).
Table 4
30 day outcomes.
All patients (n = 168)
Patients with severe CKD (n = 20)
Patients without severe CKD (n = 148)
p value
All-cause mortality
3 (1.8%)
0 (0%)
3 (2.0%)
0.68
Device success
159 (96.4%)
20 (100%)
139 (95.9%)
1.0
Early safety
150 (91%)
18 (90%)
132 (91%)
1.0
Clinical efficacy
156 (95.1%)
20 (100%)
136 (94.4%)
0.6
Any stroke
0 (0%)
0 (0%)
0 (0%)
N/A
New permanent pacemaker
6 (3.6%)
2 (10%)
4 (2.7%)
0.15
Major vascular complication
11 (6.6%)
1 (5%)
10 (6.8%)
1.0
Major or life-threatening bleeding
12 (7.1%)
1 (5%)
11 (7.4%)
1.0
CKD = chronic kidney disease Device success, early safety and clinical efficacy according to VARC2 criteria.
Discussion
We evaluated the feasibility of a novel integrated approach incorporating gadolinium-free MR instead of MSCT and administration of the bare minimum amount of CM in a cohort of patients with severe CKD and treated with TAVI. By applying this concept, we were able to reduce the total amount of CM by 64% in afflicted patients. Although the number of type 1 AKI was still slightly higher in patients with severe CKD, all other procedure-related risks appeared not to be impacted. This implicates that avoiding and reducing CM to an absolute minimum in TAVI patients is feasible and does not necessarily impact safety.
To our very best knowledge, this study is the first to select prosthesis size solely based on gadolinium-free MR. MR provided sufficient quality for annular assessment in all patients. Notably, none of the patient had moderate or severe paravalvular regurgitation, there were no strokes and there was no mortality within 30 days in patients with severe CKD. Furthermore, MR provided sufficient quality for iliofemoral artery measurements in all patients. Therefore, gadolinium-free MR may be a valuable alternative imaging modality in patients with severe CKD.
Pathophysiology of acute kidney injury
AKI following TAVI has been reported in 15‒57% of patients [11–14]. Intraprocedural episodes of hypotension, dehydration, administration of contrast media, or periprocedural bleeding may result in tubular ischemia. Furthermore, catheter manipulation and plaque rupture may result in dislodgement of plaques and cholesterol embolism [15–17]. In our study, the incidence of AKI in patients with severe CKD was 25%, but was mild (stage 1) in most. CKD may lead to chronic inflammation, oxidative stress, sympathetic nerve overactivity and thrombogenic factors thus accelerating the atherosclerotic process [18–21]. Several studies have confirmed that AKI is a strong predictor for short- and long- term mortality after TAVI [7, 22–25]. In our study including a limited number of patients with severe CKD, 30 day and 6 months survival rates were excellent.
Relevance of contrast media
The reported incidence of contrast- induced nephropathy in an unselected group of patients undergoing invasive catheterization was approximately 15% [26, 27]. In patients with additional risk factors, this incidence increased to 50% or more [28]. Previous publications have shown that administration of 100 ml contrast media for coronary interventions was associated with an increased risk of contrast- induced nepropathy, and even mortality [26, 29, 30]. Recent trials reported an average amount of contrast media for TAVI between 90 ml and 220 ml [4, 31], whereas a significant amount of CM may be additionally required for procedural planning. Using our integrated protocol in selected TAVI patients with impaired renal function may allow physicians to minimize the amount of administered CM and consequently mitigate the risk of AKI.
MR for valve selection
Correct sizing of the aortic annulus is crucial for successful valve implantation [32]. Bernhardt et al. suggested that non-enhanced MR may be used as an alternative imaging modality with similar accuracy compared to MSCT for aortic annulus measurements [33]. In the current literature is a small case series published with five patients with severe CKD who underwent TAVI without prior MSCT [34]. Valve sizing was based on echocardiography, aortography, calcification on fluoroscopy as well as weight and height of the patient and TAVI seemed to be feasible without prior dedicated imaging. The present study is the first where valve size was chosen by solely relying on MR measurements. We used a 3 dimensional MR approach with individual reconstruction of the aortic annulus at the level of the lowest hinge points of the cusps. This way, valve sizing was feasible in all patients undergoing MR. The main expected difference of MR compared with MSCT is that calcifications appear as a negative signal which can lead to an underestimation of annular and leaflet calcification with MR. In our study we used self-expanding valves in almost all patients to reduce the risk of annular rupture. Only one patient with a large aortic annulus was treated with a Sapien 3 29 mm. Interestingly, Pulerwitz et al. showed in 52 patients that MSCT with 20 ml of contrast media was in most patients of diagnostic quality for preprocedural TAVI planning [35]. Using a low contrast media MSCT protocol could be an alternative approach in patients with severe chronic kidney disease undergoing TAVI. Procedural success matched with patients who underwent pre-TAVI evaluation with a standardized MSCT protocol.
Study limitations
First, this is a relatively small, observational study lacking a control arm. Second, applicability of our integrated approach to other TAVI patients remains unknown and needs to be determined. Finally, we report a single-center experience and more prospective studies evaluating this and similar strategies are warrented.
Conclusion
In patients with severe CKD requiring TAVI, using gadolinium-free MR instead of MSCT for pre-procedural planning and periprocedural reduction of CM to a bare minimum appears feasible and safe in patients undergoing TAVI with self-expanding valves. When compared to regular TAVI patients, this integrated approach may allow a CM reduction of 64% (260±79 ml versus 94±54 ml). In this context, our study highlights that gadolinium-free MR renders adequate image quality enabling detailed TAVI procedure planning, including aortic annulus and iliofemoral arteries assessment, and finally selection of the most appropriate aortic valve prosthesis. To our best knowledge, this has not yet been described elsewhere.
Correspondence
PD Dr. Stefan Toggweiler, MD, Heart Center Lucerne, Cardiology, Spitalstrasse , CH-6000 Luzern, stefan.toggweiler[at]luks.ch
References
1Toggweiler S, Gurvitch R, Leipsic J, Wood DA, Willson AB, Binder RK, et al.Percutaneous aortic valve replacement: vascular outcomes with a fully percutaneous procedure. J Am Coll Cardiol. 2012;59(2):113–8. doi:. http://dx.doi.org/10.1016/j.jacc.2011.08.069PubMed
2Hansen JW, Foy A, Yadav P, Gilchrist IC, Kozak M, Stebbins A, et al.Death and Dialysis After Transcatheter Aortic Valve Replacement: An Analysis of the STS/ACC TVT Registry. JACC Cardiovasc Interv. 2017;10(20):2064–75. doi:. http://dx.doi.org/10.1016/j.jcin.2017.09.001PubMed
3Wenaweser P, Pilgrim T, Kadner A, Huber C, Stortecky S, Buellesfeld L, et al.Clinical outcomes of patients with severe aortic stenosis at increased surgical risk according to treatment modality. J Am Coll Cardiol. 2011;58(21):2151–62. doi:. http://dx.doi.org/10.1016/j.jacc.2011.05.063PubMed
4Yamamoto M, Hayashida K, Mouillet G, Chevalier B, Meguro K, Watanabe Y, et al.Renal function-based contrast dosing predicts acute kidney injury following transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2013;6(5):479–86. doi:. http://dx.doi.org/10.1016/j.jcin.2013.02.007PubMed
5Abdel-Wahab M, Mehilli J, Frerker C, Neumann FJ, Kurz T, Tölg R, et al.; CHOICE investigators. Comparison of balloon-expandable vs self-expandable valves in patients undergoing transcatheter aortic valve replacement: the CHOICE randomized clinical trial. JAMA. 2014;311(15):1503–14. doi:. http://dx.doi.org/10.1001/jama.2014.3316PubMed
6Madershahian N, Scherner M, Liakopoulos O, Rahmanian P, Kuhn E, Hellmich M, et al.Renal impairment and transapical aortic valve implantation: impact of contrast medium dose on kidney function and survival. Eur J Cardiothorac Surg. 2012;41(6):1225–32. doi:. http://dx.doi.org/10.1093/ejcts/ezr199PubMed
7Bagur R, Webb JG, Nietlispach F, Dumont E, De Larochellière R, Doyle D, et al.Acute kidney injury following transcatheter aortic valve implantation: predictive factors, prognostic value, and comparison with surgical aortic valve replacement. Eur Heart J. 2010;31(7):865–74. doi:. http://dx.doi.org/10.1093/eurheartj/ehp552PubMed
8Meneguz-Moreno RA, Ramos AI, Siqueira D, de Castro-Filho A, Jatene T, Dias Jeronimo A, et al.Prognostic value of renal function in patients with aortic stenosis treated with transcatheter aortic valve replacement. Catheter Cardiovasc Interv. 2017;89(3):452–9. doi:. http://dx.doi.org/10.1002/ccd.26693PubMed
10Khalique OK, Pulerwitz TC, Halliburton SS, Kodali SK, Hahn RT, Nazif TM, et al.Practical considerations for optimizing cardiac computed tomography protocols for comprehensive acquisition prior to transcatheter aortic valve replacement. J Cardiovasc Comput Tomogr. 2016;10(5):364–74. doi:. http://dx.doi.org/10.1016/j.jcct.2016.07.007PubMed
11Thamcharoen N, Thongprayoon C, Edmonds PJ, Cheungpasitporn W. Periprocedural Nebivolol for the Prevention of Contrast-Induced Acute Kidney Injury: A Systematic Review and Meta-analysis. N Am J Med Sci. 2015;7(10):446–51. doi:. http://dx.doi.org/10.4103/1947-2714.168670PubMed
12Elhmidi Y, Bleiziffer S, Deutsch MA, Krane M, Mazzitelli D, Lange R, et al.Acute kidney injury after transcatheter aortic valve implantation: incidence, predictors and impact on mortality. Arch Cardiovasc Dis. 2014;107(2):133–9. doi:. http://dx.doi.org/10.1016/j.acvd.2014.01.002PubMed
13Wenaweser P, Pilgrim T, Guerios E, Stortecky S, Huber C, Khattab AA, et al. Impact of coronary artery disease and percutaneous coronary intervention on outcomes in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation. EuroIntervention. 2011;7(5):541-8. http://dx.doi.org/10.3109/14017431.2012.699636PubMed
14Appel CF, Hultkvist H, Nylander E, Ahn H, Nielsen NE, Freter W, et al.Transcatheter versus surgical treatment for aortic stenosis: patient selection and early outcome. Scand Cardiovasc J. 2012;46(5):301–7. doi:. http://dx.doi.org/10.3109/14017431.2012.699636PubMed
15Najjar M, Salna M, George I. Acute kidney injury after aortic valve replacement: incidence, risk factors and outcomes. Expert Rev Cardiovasc Ther. 2015;13(3):301–16. doi:. http://dx.doi.org/10.1586/14779072.2015.1002467PubMed
16Aikawa E, Aikawa M, Libby P, Figueiredo JL, Rusanescu G, Iwamoto Y, et al.Arterial and aortic valve calcification abolished by elastolytic cathepsin S deficiency in chronic renal disease. Circulation. 2009;119(13):1785–94. doi:. http://dx.doi.org/10.1161/CIRCULATIONAHA.108.827972PubMed
17Scolari F, Ravani P, Gaggi R, Santostefano M, Rollino C, Stabellini N, et al.The challenge of diagnosing atheroembolic renal disease: clinical features and prognostic factors. Circulation. 2007;116(3):298–304. doi:. http://dx.doi.org/10.1161/CIRCULATIONAHA.106.680991PubMed
19Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–305. doi:. http://dx.doi.org/10.1056/NEJMoa041031PubMed
20Massy ZA, Ivanovski O, Nguyen-Khoa T, Angulo J, Szumilak D, Mothu N, et al.Uremia accelerates both atherosclerosis and arterial calcification in apolipoprotein E knockout mice. J Am Soc Nephrol. 2005;16(1):109–16. doi:. http://dx.doi.org/10.1681/ASN.2004060495PubMed
21Schwarz U, Buzello M, Ritz E, Stein G, Raabe G, Wiest G, et al.Morphology of coronary atherosclerotic lesions in patients with end-stage renal failure. Nephrol Dial Transplant. 2000;15(2):218–23. doi:. http://dx.doi.org/10.1093/ndt/15.2.218PubMed
22Elhmidi Y, Bleiziffer S, Piazza N, Hutter A, Opitz A, Hettich I, et al.Incidence and predictors of acute kidney injury in patients undergoing transcatheter aortic valve implantation. Am Heart J. 2011;161(4):735–9. doi:. http://dx.doi.org/10.1016/j.ahj.2011.01.009PubMed
23Nuis RJ, Van Mieghem NM, Tzikas A, Piazza N, Otten AM, Cheng J, et al.Frequency, determinants, and prognostic effects of acute kidney injury and red blood cell transfusion in patients undergoing transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2011;77(6):881–9. doi:. http://dx.doi.org/10.1002/ccd.22874PubMed
24Barbash IM, Ben-Dor I, Dvir D, Maluenda G, Xue Z, Torguson R, et al.Incidence and predictors of acute kidney injury after transcatheter aortic valve replacement. Am Heart J. 2012;163(6):1031–6. doi:. http://dx.doi.org/10.1016/j.ahj.2012.01.009PubMed
25Khawaja MZ, Thomas M, Joshi A, Asrress KN, Wilson K, Bolter K, et al.The effects of VARC-defined acute kidney injury after transcatheter aortic valve implantation (TAVI) using the Edwards bioprosthesis. EuroIntervention. 2012;8(5):563–70. doi:. http://dx.doi.org/10.4244/EIJV8I5A87PubMed
26McCullough PA, Wolyn R, Rocher LL, Levin RN, O’Neill WW. Acute renal failure after coronary intervention: incidence, risk factors, and relationship to mortality. Am J Med. 1997;103(5):368–75. doi:. http://dx.doi.org/10.1016/S0002-9343(97)00150-2PubMed
27Iakovou I, Dangas G, Mehran R, Lansky AJ, Ashby DT, Fahy M, et al.Impact of gender on the incidence and outcome of contrast-induced nephropathy after percutaneous coronary intervention. J Invasive Cardiol. 2003;15(1):18–22. PubMed
28McCullough PA, Adam A, Becker CR, Davidson C, Lameire N, Stacul F, et al.; CIN Consensus Working Panel. Risk prediction of contrast-induced nephropathy. Am J Cardiol. 2006;98(6A):27K–36K. doi:. http://dx.doi.org/10.1016/j.amjcard.2006.01.022PubMed
29Mehran R, Aymong ED, Nikolsky E, Lasic Z, Iakovou I, Fahy M, et al.A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44(7):1393–9. doi:. http://dx.doi.org/10.1016/j.jacc.2004.06.068PubMed
30Rihal CS, Textor SC, Grill DE, Berger PB, Ting HH, Best PJ, et al.Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002;105(19):2259–64. doi:. http://dx.doi.org/10.1161/01.CIR.0000016043.87291.33PubMed
31Wöhrle J, Gonska B, Rodewald C, Trepte U, Koch S, Scharnbeck D, et al.Transfemoral aortic valve implantation with the repositionable Lotus valve compared with the balloon-expandable Edwards Sapien 3 valve. Int J Cardiol. 2015;195:171–5. doi:. http://dx.doi.org/10.1016/j.ijcard.2015.05.139PubMed
32Willson AB, Webb JG, Labounty TM, Achenbach S, Moss R, Wheeler M, et al.3-dimensional aortic annular assessment by multidetector computed tomography predicts moderate or severe paravalvular regurgitation after transcatheter aortic valve replacement: a multicenter retrospective analysis. J Am Coll Cardiol. 2012;59(14):1287–94. doi:. http://dx.doi.org/10.1016/j.jacc.2011.12.015PubMed
33Bernhardt P, Rodewald C, Seeger J, Gonska B, Buckert D, Radermacher M, et al.Non-contrast-enhanced magnetic resonance angiography is equal to contrast-enhanced multislice computed tomography for correct aortic sizing before transcatheter aortic valve implantation. Clin Res Cardiol. 2016;105(3):273–8. doi:. http://dx.doi.org/10.1007/s00392-015-0920-6PubMed
34Arrigo M, Maisano F, Haueis S, Binder RK, Taramasso M, Nietlispach F. Transcatheter aortic-valve implantation with one single minimal contrast media injection. Catheter Cardiovasc Interv. 2015;85(7):1248–53. doi:. http://dx.doi.org/10.1002/ccd.25799PubMed
35Pulerwitz TC, Khalique OK, Nazif TN, Rozenshtein A, Pearson GD, Hahn RT, et al.Very low intravenous contrast volume protocol for computed tomography angiography providing comprehensive cardiac and vascular assessment prior to transcatheter aortic valve replacement in patients with chronic kidney disease. J Cardiovasc Comput Tomogr. 2016;10(4):316–21. doi:. http://dx.doi.org/10.1016/j.jcct.2016.03.005PubMed
36Kappetein AP, Head SJ, Généreux P, Piazza N, van Mieghem NM, Blackstone EH, et al.Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. J Am Coll Cardiol. 2012;60(15):1438–54. doi:. http://dx.doi.org/10.1016/j.jacc.2012.09.001PubMed