Chagas heart disease is becoming a worldwide health burden and represents a major cause of cardiovascular death in areas where it is endemic.
Introduction
Chagas heart disease, a form of a dilated cardiomyopathy caused by Trypanosoma cruzi, is a major cause of cardiovascular related death in endemic areas. Although Chagas disease occurs significantly less often in Switzerland, physicians should be aware of the disease, especially in times of increased migration and mobility.
Chagas heart disease involves progressive myocardial fibrosis, left ventricular dilatation and dysfunction, ventricular aneurysm, congestive heart failure, thromboembolism, ventricular arrhythmias, cardiac conduction system abnormalities and sudden cardiac death, which is the main cause of death in patients with Chagas heart disease.
This article describes a rare case of Chagas heart disease in a young woman in Switzerland and gives an overview of the disease including diagnosis, treatment and prognosis.
Case description
Patient history
A 45-year-old woman was referred by her general practitioner to the emergency department because of progressive dyspnoea and newly diagnosed left bundle branch (LBBB) on electrocardiogram (ECG). The patient was working as a home-care nurse and reported acute onset of dyspnoea for 4 days and chest discomfort. Her only medication was levothyroxine, which she was taking for hypothyroidism. The remaining medical history was unremarkable. There were no cardiovascular risk factors and no history of cardiotoxic medication, but she reported a notable family history. An uncle and two aunts died at age 45 and 50 years, respectively, of sudden cardiac death. Autopsies had revealed acute myocardial infarction, according to the patient. She was born in Brazil and grew up on a farm. She lived in Switzerland from 1993 to 2000 and moved back to Brazil from 2000 to 2013. In 2013 she moved back to Switzerland and has lived here since.
Diagnostic assessment
The physical examination showed a haemodynamically stable patient with signs of volume overload and mild respiratory distress.
The ECG revealed sinus rhythm with normal atrioventricular conduction, LBBB and peripheral low voltage. Chest X-ray showed cardiomegaly and cardiopulmonary hypervascularity with bilateral pleural effusions.
High sensitivity troponin and creatinine kinase were normal. Brain natriuretic peptide was elevated at 815 ng/l (reference range <111 ng/l). Thyroid stimulating hormone was also elevated (11.6 mU/l, reference range 0.35–4.94 mU/l); however, free thyroid hormones were normal (table 1).
Because of a high pretest probability of pulmonary embolism, a computed tomography (CT) scan was performed, which ruled out pulmonary embolism and aortic dissection.
Transthoracic echocardiography showed a dilated left ventricle with a severely impaired left ventricular function (ejection fraction [EF] 25%), diffuse hypokinesia and thinning of the septal myocardium, but without apical ballooning. This made a typical Takotsubo cardiomyopathy, a differential diagnosis of acute chest pain and poor left ventricular function in a young female, unlikely. The right ventricle was normal in size, but with reduced function.
Because of the persistent dyspnoea, we performed a thoracentesis, which showed a transudate.
To exclude ischaemic heart disease, the most common cause of heart failure, we performed coronary angiography, which showed unobstructed coronaries.
Laboratory test results indicated that acute viral perimyocarditis, human immunodeficiency virus infection, hepatitis, syphilis, connective tissue disorders, vasculitis and cardiomyopathy related to renal disease were unlikely (table 1). Further, normal levels of ferritin and angiotensin converting enzyme excluded haemochromatosis and sarcoidosis. Free light chains, a marker for amyloidosis, were negative in the serum and urine.
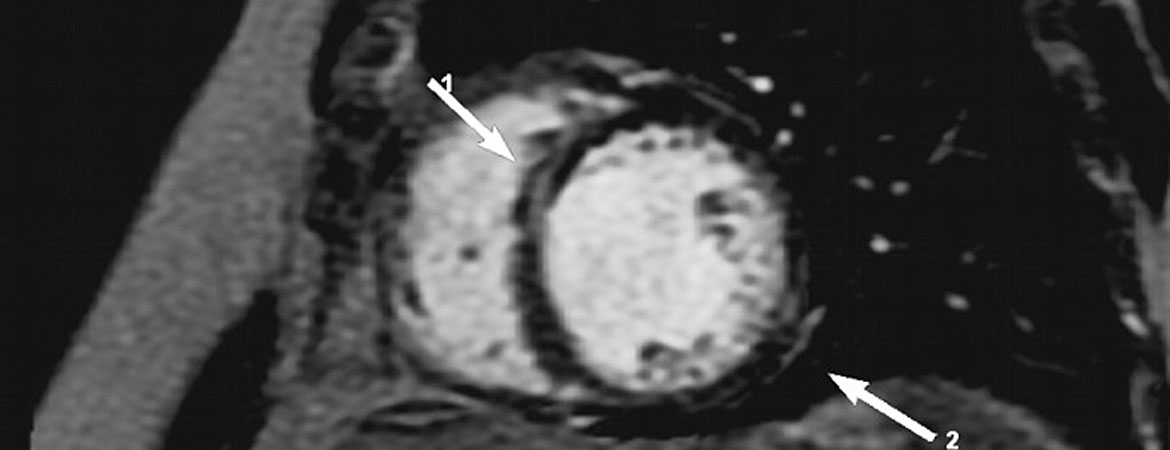
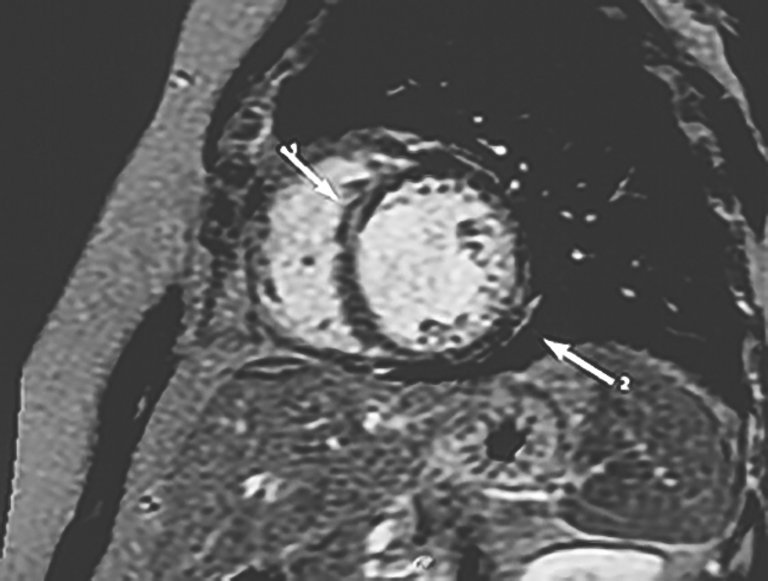
Subsequent cardiac magnetic resonance imaging (CMR) showed a dilated left ventricle with diffuse hypokinesia, but an already improved EF of 40%. There was no oedema within the myocardium, but late gadolinium enhancement was present in the septum and the lateral epicardial wall (fig. 1).
Figure 1: CMR with late gadolinium enhancement in the septum (1) and lateral wall epicardially (2) (marked by arrows).
Owing to the patient’s ethnicity, Chagas disease was considered at an early stage in the investigations and accordingly samples were sent to an external laboratory (Swiss Tropical and Public Health Institute in Basel), although the patient did not recall having had an acute Trypanosoma infection in childhood or later in her life. Tests for IgG against T. cruzi by enzyme-linked immunosorbent assay and indirect immunofluorescence antibody test were positive, confirming Chagas disease.
Treatment
We immediately began intravenous diuretic therapy with furosemide and initiated standard therapy for heart failure. In addition, we modified the dose of levothyroxine. Dyspnoea resolved with intravenous diuretic therapy. After installation of heart failure treatment, the left ventricular ejection fraction (LVEF)improved from 25 to 40% and remained stable during follow-up. Because of the risk of arrhythmias in Chagas cardiomyopathy and poor left ventricular function at the baseline, we initially discharged the patient with a portable defibrillator (Life Vest®). Because of the late stage chronic Chagas disease at presentation, antiparasitic therapy was not recommended by the guidelines. The patient was instructed to have her daughter tested for Chagas disease because of the possibility of antiparasitic treatment. Further, we instructed the patient to use contraceptives to avoid pregnancy because of heart failure and the possibility of parasitic transmission to the fetus. She was also warned to avoid blood donation.
Follow-up and outcome
The portable defibrillator analysis showed no relevant arrhythmias within the first 3 months after diagnosis. After three months of Life Vest® protection, an electrophysiological study was performed, mainly to assess atrioventricular conduction in view of LBBB in Chagas heart disease, and was normal. No ventricular arrhythmias could be induced. During the electrophysiological study we saw episodes of atrial fibrillation, which started after atrial pacing and were self-limiting. At that point, the clinical relevance of this artificially induced arrhythmia was unclear; atrial fibrillation was not observed either during her stay in the hospital or during Life Vest® monitoring. Thus, oral anticoagulation was not prescribed. At that point there was no indication for a pacemaker or implantable defibrillator (ICD). For further arrhythmia monitoring and detection (especially heart block, ventricular tachycardia or atrial fibrillation, as these are common in Chagas heart disease) an implantable loop recorder (ILR) was fitted (Medtronic Reveal®). The subsequent ILR checks have been unremarkable so far.
With an increased dosage of heart failure therapy with repeated adjustments of diuretics, the clinical status of the patient remained stable.
Discussion
Chagas disease was discovered in 1909 by the Brazilian physician Carlos Chagas and is caused by T. cruzi, a protozoan parasite that can cause acute cardiac infection (perimyocarditis) as well as chronic myocardial fibrosis [1]. T. cruzi is transmitted to humans through the faeces of infected triatomine bugs, deposited during the blood meal and most commonly when a bitten person rubs infective faeces into the bite wound while scratching the area. T. cruzi can occasionally be transmitted by non-vectorial mechanisms such as blood transfusion [2] or vertically from mother to fetus [3]. Rarely, Chagas disease can be contracted by ingestion of contaminated food or liquids, which is generally associated with a massive parasitic infestation, resulting in a more severe acute clinical presentation and high mortality [3].
The disease is endemic in South America, especially in Argentina, Bolivia, Brazil, Chile, Uruguay and Venezuela. It is estimated that 100 million individuals are at risk of infection and 16 to 18 million are affected by Chagas disease [1], which is a major cause of heart failure and cardiovascular death in this area [4]. Chagas disease is reported to be rare in Europe, but the incidence is increasing owing to demographic changes and travel. Nearly 36.2 million tourists have been to South America in 2017 according to official statistics by the World Tourism Organization of the United Nations. Such tourists may have been in contact with the vector.
Europe currently has a large population of migrants. A systematic review indicated that 4.2% of Latin American individuals living in European countries have chronic Chagas disease [4]. In Switzerland, 22.4% of the total population of 7.8 million inhabitants were foreigners in 2010; 35,000 were Latin American migrants from 21 endemic countries. Between 1979 and 2011, 258 cases of Chagas disease were diagnosed in Switzerland, mostly after 2008 when a wider screening-strategy for Chagas disease was implemented in Geneva because of the local high numbers of Latin American immigrants, especially Bolivians. The prevalence might be underestimated, because many of the migrants from the disease-affected areas are without a residence permit or health insurance (176 of the 258 diagnosed cases) [5].
The acute, indeterminate and chronic infection:
The acute phase of the disease begins 1 to 2 weeks after inoculation and lasts for 4 to 8 weeks. After that period, individuals enter the indeterminate phase, which is characterised by chronic asymptomatic infection [1, 3].
In most individuals, acute Chagas infection is usually asymptomatic. When symptoms occur, they first include local inflammation at the parasite entry site (which is called Chagoma when entry is through skin, or the Romaña sign when entry is via ocular mucous membranes, which causes a characteristic swelling of the eyelid), malaise, fever, and enlargement of the liver, spleen and lymph nodes. Approximately 5% of these patients develop fatal complications, including acute heart failure, arrhythmia or meningoencephalitis [1, 3]. Treatment with an antiparasitic drug, such as benznidazole, will usually cure the acute infection and prevent chronic manifestations [3].
Because of the nonspecific symptoms of acute Chagas disease and the lack of access of poor patients to medical care, the illness is underdiagnosed. The manifestations of acute disease resolve spontaneously in about 90% of cases, which leads to the indeterminate form of chronic Chagas disease characterised by positivity of tests for antibodies against T. cruzi in serum, but a normal 12-lead ECG and normal radiological examinations of chest, oesophagus and colon. About 60 to 70% of the patients remain in the indeterminate form of chronic Chagas disease. However, 30 to 40% subsequently develop a determinate form of chronic Chagas disease after 10 to 30 years, with involvement of the heart, oesophagus (megaoesophagus), colon (megacolon) or all of these [1, 3].
Chronic Chagas heart disease includes left ventricular dilatation and dysfunction, aneurysm, congestive heart failure, thromboembolism, ventricular arrhythmias, cardiac conduction system abnormalities (most commonly sick sinus syndrome and second- and third-degree atrioventricular block with bundle branch block) and sudden cardiac death, which is the main cause of death in patients with Chagas heart disease, accounting for nearly two-thirds of all deaths [1, 3].
Diagnostic evaluation of Chagas disease
The diagnosis of acute infections is made by detection of circulating trypomastigotes in the blood [3].
The diagnosis of chronic Chagas disease is based on demonstration of antibodies directed against T. cruzi antigens by at least two different serological tests and a clinical syndrome compatible with the disease. The most commonly used serological tests are an enzyme-linked immunosorbent assay, indirect immunofluorescence and indirect haemagglutination [1]. A 12-lead ECG and evaluation of gastrointestinal symptoms are needed to define whether there is an indeterminate, cardiac, digestive or a mixed form of Chagas disease. An abnormal ECG with many premature ventricular beats, bundle branch block, T wave inversion, abnormal Q waves, variable atrioventricular block and low voltage of QRS requires further cardiac assessment by chest radiography, echocardiography and 24-hour ECG monitoring for further classification of the cardiac stage [1, 3].
According to the current European Association of Cardiovascular Imaging (EACVI) expert consensus from 2017, echocardiography may demonstrate diastolic dysfunction in early cardiac stages. Segmental left ventricular wall motion abnormalities may be present, more frequently in the inferior and inferolateral walls and the apex region. This may range from mild wall motion abnormalities to aneurysm formation. Apical aneurysm is typical in Chagas disease, but localisation is not limited to the apex alone. However, our patient did not show any aneurysm formation. In cases of unsatisfactory echo quality, application of contrast echocardiography or additional CMR is highly recommended by the current consensus of experts, as it may better demonstrate the wall motion abnormities and LVEF [6]. CMR should also be considered to quantify the extent of myocardial fibrosis through late gadolinium enhancement. Late gadolinium enhancement is heterogeneous in Chagas cardiomyopathy, sometimes even located epicardially, making ablation treatment of arrhythmias such ventricular tachycardia by technically challenging.
Antitrypanosomal treatment
Two antiparasitic drugs are available for treatment of Chagas disease (benznidazole and nifurtimox). Antitrypanosomal treatment is strongly recommended for all cases of acute, congenital or reactivated infection, including infected children and patients up to 18 years of age with chronic disease. Drug treatment can be offered to adults aged 19 to 50 years without advanced Chagas heart disease. However, evidence of benefit with antiparasitic treatment in adults above 50 years in the chronic stage of infection and with established cardiomyopathy is limited, because of the lack of effect in reducing clinical progression of cardiac disease [7, 8]. Antitrypanosomal treatment is contraindicated during pregnancy and in patients with severe renal or hepatic insufficiency [3].
Treatment of cardiac symptoms
Management of ventricular dysfunction and heart failure
Patients with Chagas-related heart failure should receive an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker and adrenergic beta-blockers to reduce mortality. Diuretics are indicated in the case of volume overload. According to guidelines of the Brazilian Society of Cardiology, digoxin may be considered in cases of atrial fibrillation [9].
The European Society of Cardiology (ESC) recommends the use of spironolactone in patients who have heart failure with a LVEF <35% and heart failure symptoms, for mortality reduction. Spironolactone may also be helpful owing to the major role of cardiac fibrosis in Chagas heart disease [1].
Cardiac resynchronisation therapy is recommended by the ESC guidelines for patients who have heart failure with LVEF <35% and QRS width of at least 130 ms. A trial showed that cardiac resynchronisation therapy in selected Chagas heart disease patients led to LVEF improvement (from 28 ± 5% to 32.2 ± 11%) and a reduction in New York Heart Association (NYHA) functional class (from 3.5 ± 0.5 to 2.5 ± 0.8) [10, 11].
Heart transplantation is the only option for patients with end-stage heart failure after failed pharmacological and device therapy. Promising results were found in some cases [1, 12]. However, patients must be treated with antitrypanosomal agents, because of the possibility of T. cruzi infection reactivation after concomitant use of immunosuppressive drugs [1].
Management of bradyarrhythmias
Sinus and atrioventricular node dysfunction, which may be heralded by bundle branch block, are frequent in Chagas heart disease. Complete atrioventricular block in chronic Chagas disease has already been reported in Switzerland [13]. Indications for pacemaker implantation follow usual recommendations by current guidelines. To prevent failure of pacing by exit block, the lead should be placed in the subtricuspid area and not in the right ventricular apex, because of common apical fibrosis in Chagas heart disease [1].
Management of ventricular arrhythmias
As indicated by the review of Muratore et al., ventricular arrhythmias are usually not sustained, but may indicate risk of sudden cardiac death, usually due to ventricular fibrillation, which is the cause of death in up to 51 to 65% of affected patients [10]. Two trials (one prospective and placebo-controlled, the other open, parallel, randomised and experimental) have shown that amiodarone is the most effective antiarrhythmic agent and is well tolerated [14, 15]. The rate of recurrence of ventricular tachycardia often remains high, despite best possible treatment. In this case, radiofrequency ablation, endo- and potentially epicardially (epicardial involvement is common in Chagas), has been shown to reduce the recurrence of ventricular tachycardia [10].
Implantation of an internal cardiac defibrillator (ICD) should be considered for patients with refractory and haemodynamically unstable sustained ventricular tachycardia, for survivors of sudden cardiac arrest and patients with a classic indication for primary prophylactic implantation for heart failure, as recommended by current guidelines [1].
Management of chest pain
Chest pain may be a manifestation of Chagas heart disease. Myocardial microvessel abnormalities are postulated as pathophysiological substrate [6, 16]. Differential diagnosis should include assessment of associated ischaemic heart disease, for example by coronary catheterisation, coronary CT angiography, or CMR [16].
Management of thromboembolism
Oral anticoagulation is indicated in patients with chronic Chagas heart disease who develop atrial fibrillation or mural thrombus, usually after aneurysm formation. Oral anticoagulation is a class I recommendation of the Brazil Society of Cardiology for patients with previous embolic cerebrovascular events, because of the high annual incidence of thromboembolic events of up to 1 to 2% in Chagas heart disease[9].
Prognostic markers and risk stratification in chronic Chagas heart disease
The Rassi score may help to predict total long-term mortality in affected patients. The strongest and most consistent predictors of mortality are presented in table 2. A score of 0 to 6 points represents a low risk with a 5-year mortality of 2% and 10-year mortality of 10%. At intermediate risk are patients with 7 to 11 points, who have a 5-year mortality of 18% and a 10-year mortality of 44%. A score of 12 to 20 points predicts a 5-year mortality of 63% and a 10 year-mortality of 84% (high risk) [17].
Table 2: Rassi risk score for total long-term mortality in affected patients.
Predictors of mortality
Points
New York Heart Association functional class III or IV
5
Cardiomegaly on chest radiography
5
Segmental or global wall motion abnormality
3
Non-sustained ventricular tachycardia on 24-hour ECG monitoring
2
Male sex
2
Maximum total
17
Take-home messages
1. Dilated cardiomyopathy is often idiopathic; however searching for specific causes is crucial as therapy may differ from simple heart failure treatment
2. Clinicians should be aware of Chagas disease, which has become more relevant due to migration and travel, as a cause for dilated cardiomyopathy in Europe.
3. The diagnosis of the chronic disease is established via a compatible clinical presentation (cardiac, digestive or cardio-digestive) and detection of antibodies against T. cruzi antigens with least two different serological tests.
4. Acute Chagas disease must be treated with antiparasitic medication. Antiparasitic treatment in chronic Chagas disease depends on the patient’s age and how advanced the disease is.
Informed consent
The authors confirm that written consent for submission and publication of this case report including images and associated text has been obtained from the patient in line with COPE guidance.
Disclosure statement
No financial support and no other potential conflict of interest relevant to this article was reported.
Correspondence
Correspondence: Deborah Schild, MD Department of Cardiology Buergerspital Solothurn Schoengruenstrasse 42 CH-4500 Solothurn deborah.schild[at]spital.so.ch
2 Ries J, Komarek A, Gottschalk J, Brand B, Amsler L, Jutzi M, et al. A Case of Possible Chagas Transmission by Blood Transfusion in Switzerland. Transfus Med Hemother. 2016;43(6):415–7. doi:https://doi.org/10.1159/000446264.
5 Jackson Y, Chappuis F. Chagas disease in Switzerland: history and challenges. Euro Surveill. 2011;16(37):19963.
6 Nunes MCP, Badano LP, Marin-Neto JA, Edvardsen T, Fernández-Golfín C, Bicciarelli-Ducci C, et al. Multimodality imaging evaluation of Chagas disease: an expert consensus of Brazilian Cardiovascular Imaging Department (DIC) and the European Association of Cardiovascular Imaging (EACVI). Eur Heart J Cardiovasc Imaging. 2018;19(4):459–60.
7 Viotti R, Vigliano C, Lococo B, Bertocchi G, Petti M, Alvarez MG, et al. Long-term cardiac outcomes of treating chronic Chagas disease with benznidazole versus no treatment: a nonrandomized trial. Ann Intern Med. 2006;144(10):724–34. doi:https://doi.org/10.7326/0003-4819-144-10-200605160-00006.
8 Morillo CA, Marin-Neto JA, Avezum A, Sosa-Estani S, Rassi A, Jr, Rosas F, et al.; BENEFIT Investigators. Randomized Trial of Benznidazole for Chronic Chagas’ Cardiomyopathy. N Engl J Med. 2015;373(14):1295–306. doi:https://doi.org/10.1056/NEJMoa1507574.
9 Andrade JP, Marin-Neto JA, Paola AA, Vilas-Boas F, Oliveira GM, Bacal F, et al., Sociedade Brasileira de Cardiologia. I Diretriz Latino Americana para o Diagnóstico e Tratamento da Cardiopatia Chagásica. Diretriz Latino-Americana para o Diagnóstico e Tratamento da Cardiopatia Chagásica [Latin American guidelines for the diagnosis and treatment of Chagas cardiomyopathy]. Arq Bras Cardiol. 2011;97(2, Suppl 3):1–48. Article in Protugese. doi:https://doi.org/10.1590/S0066-782X2011001600001.
10 Muratore CA, Baranchuk A. Current and emerging therapeutic options for the treatment of chronic chagasic cardiomyopathy. Vasc Health Risk Manag. 2010;6:593–601. doi:https://doi.org/10.2147/VHRM.S8355.
11 Alves Fagundes A, Latado Braga A, Pereira Magalhaes L. Impacto da terapia de ressincronizacao cardíaca na cardiopatía chagásica. Rev Latino Americana MCP y Arritmias. 2009;22(4):243.
13 Keusch S, Stämpfli SF, Hufschmid U, Beer JH, Friedli FC. Blocking bug - complete atrioventricular block in chronic Chagas disease. Cardiovasc Med. 2012;15(12):362–4. doi:https://doi.org/10.4414/cvm.2012.00130.
14 Haedo AH, Chiale PA, Bandieri JD, Lázzari JO, Elizari MV, Rosenbaum MB. Comparative antiarrhythmic efficacy of verapamil, 17-monochloracetylajmaline, mexiletine and amiodarone in patients with severe chagasic myocarditis: relation with the underlying arrhythmogenic mechanisms. J Am Coll Cardiol. 1986;7(5):1114–20. doi:https://doi.org/10.1016/S0735-1097(86)80232-7.
15 Rosenbaum M, Posse R, Sgammini H, Núñez Burgos J, Chiale PA, Pastori JD, et al. Estudio clínico multicéntrico comparativeo de la flecainida y la amiodarona en el tratamiento de las arritmias ventriculares asociadas a la cardiopatía chagásica cronica [Comparative multicenter clinical study of flecainide and amiodarone in the treatment of ventricular arrhythmias associated with chronic Chagas cardiopathy]. Arch Inst Cardiol Mex. 1987;57(4):325–30. Article in Spanish.
16 Gascón J, Albajar P, Cañas E, Flores M, Gómez i Prat J, Herrera RN, et al. Diagnóstico, manejo y tratamiento de la cardiopatía chagásica crónica en áreas donde la infección por Trypanosoma cruzi no es endémica [Diagnosis, management and treatment of chronic Chagas’ heart disease in areas where Trypanosoma cruzi infection is not endemic]. Rev Esp Cardiol. 2007;60(3):285–93. Article in Spanish.
17 Rassi A, Jr, Rassi A, Little WC, Xavier SS, Rassi SG, Rassi AG, et al. Development and validation of a risk score for predicting death in Chagas’ heart disease. N Engl J Med. 2006;355(8):799–808. doi:https://doi.org/10.1056/NEJMoa053241.