Cardiovascularmagnetic resonance imaging (CMR)is increasingly used in modern cardiology to complement the diagnostic work-up of patients with cardiovascular diseases,and to contribute torisk stratification and patientmanagement.
This casereportdescribes the pivotal role of CMR in a patient with myocardial infarction and unobstructed coronary arteries (MINOCA).
Case report
A 72-year-old woman presented to the emergency department with intense crushingcentral chestpain for 3 days,notradiatingtoarms/jaw, and not associated with exercise. She had no fever. Troponin I was elevated at 3.57 ng/l on admission, and reached a peak value 3.88 ng/ml (normal range <0.09 ng/l). Creatinine phosphokinase concentration was 155 U/I (normal range <170 U/l) and the C-reactive protein level was 46 mg/l (normal range <5 mg/l).
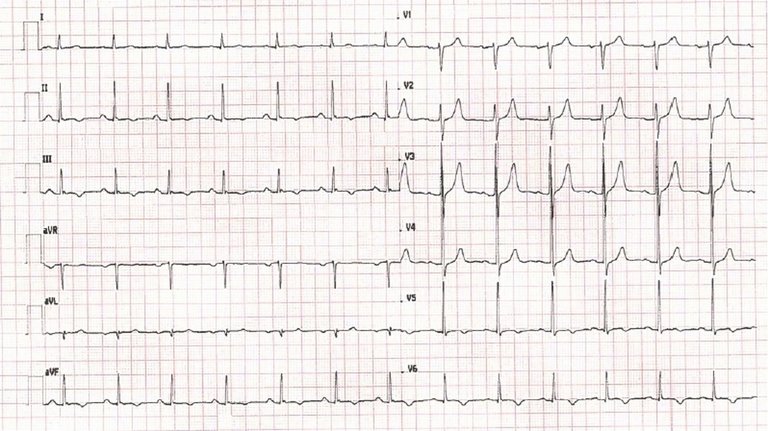
A 12-lead electrocardiogram (ECG) on admission showed normal sinus rhythm with a heart rate of 94 bpm and ST abnormalities with a negative T wave in the inferior leads and V5–V6 (fig. 1). Transthoracic echocardiography revealed mild hypokinesia of the basal and mid-cavity lateral wall, with a normal overall ejection fraction (EF) of 60%, and no pericardial effusion.
Figure 1: 12-lead ECG on admission showing normal sinus rhythm with a heart rate of 94 bpm, abnormal ST-segment and negative T-wave in inferior leads and V5–V6.
In view of the acute coronary syndrome and regional wall motion abnormalities, the patient underwent invasive angiography, which showed unobstructed coronary arteries (fig. 2 A,B,C).
Figure 2: Invasive angiography showing: (A) unobstructed right coronary artery; (B) unobstructed left main and the circumflex coronary arteries; (C) unobstructed left coronary artery.
She was then discharged with a diagnosis of acute myocarditis and referred for CMR for confirmation of the diagnosis.
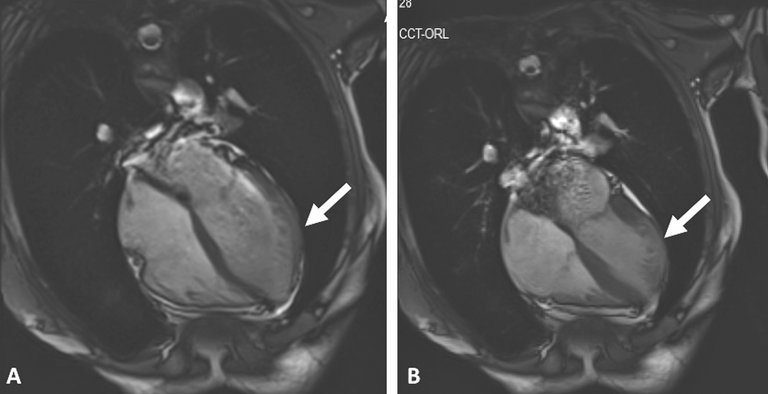
CMR was performed on a 3T system (Skyra, Siemens Medical Solutions, Erlangen, Germany). The cine CMR images confirmed the persistence of regional wall motion abnormalities in the lateral wall and global EF of 56% (fig. 3 A,B).
Figure 3: Four-chamber cine, end-diastolic (A) and end-systolic frame (B). There is an area of reduced thickening corresponding to the area of regional wall motion abnormality (white arrow).
Advanced myocardial tissue characterisation with T1 and T2 mapping confirmed the abnormal value myocardial signal intensity (T2 mapping: 60 ms, normal range in our lab <45 ms; T1 mapping: 1600 ms, normal range for our lab is <1200 ms) suggesting myocardial oedema in the region of wall motion abnormality (fig. 4 A,B).
Figure 4: CMR multi-parametric tissue characterisation, 4-chamber view: (A) T2 mapping image demonstrating an area of increased signal intensity (myocardial oedema, white arrow); (B) corresponding T1 mapping image demonstrating an area of increased signal intensity (myocardial oedema and scarring, white arrow); and (C) LGE demonstrating a transmural myocardial infarction in the lateral wall (white arrow).
Late gadolinium enhancement (LGE) images acquired after administration of a contrast agent revealed transmural LGE of the left ventricular mid-anterolateral wall (fig. 4 C). Overall, these findings suggested a recent myocardial infarction in the territory the obtuse marginal branches of the circumflex artery. In view of the unobstructed coronary arteries, this is likely to represent myocardial infarction with spontaneous recanalisation.
On the basis of the CMR findings, the final discharge diagnosis was changed from myocarditis to acute myocardial infarction and the patient was started on secondary prevention medications accordingly.
Discussion
MINOCA is not infrequent, and found on urgent angiography in 7–10% of patients presenting with ST elevation myocardial infarction (STEMI) and in 10–15% of patients presenting with non-STEMI [1]. These patients represent a clinical dilemma and the discharge diagnosis and clinical management is often challenging.
CMR plays a pivotal role in cardiac morphological and functional assessment and tissue characterisation, and has the potential to identify underlying aetiologies and aid a final diagnosis [2]. The three most common differential diagnoses of MINOCA include acute myocarditis, embolic and spontaneous recanalisation myocardial infarction, and Tako-Tsubo cardiomyopathy.
CMR provides a unique opportunity to noninvasively characterise heart tissue (oedema/inflammation and myocardial scar/fibrosis). Currently, myocardial tissue characterisation by CMR is most commonly performed with the LGE technique after contrast administration. However, novel non-contrast techniques, such as T2 and T1 mapping [3], play an increasing role in clinical practice, complementing the information acquired with the standard cine and LGE techniques without the need of a contrast agent.
Conclusion
CMR has a pivotal role in defining the underlying diagnosis in patients with MINOCA, with subsequent implication for the patients’ management and prognosis [4].
T1 and T2 mapping are novel CMR sequences that allow the detection of myocardial oedema and scarring, obviating for the need of a contrast agent. In addition, native T1 mapping in combination with T2 mapping are useful to differentiate acute from chronic myocardial infarction, and infarcted from normal myocardium.
This case illustrates the increasing clinical role of CMR in modern cardiology and its ability to detect a final diagnosis with clear implications for clinical management.
Disclosure statement
No financial support and no other potential conflict of interest relevant to this article was reported.
Correspondence
Correspondence: MD Vera Lucia Paiocchi Cardiocentro Ticino Via Tesserete 48 CH-6900 Lugano vera.paiocchi[at] cardiocentro.org
References
1 Sheikh AR, Sidharta S, Worthley MI, Yeend R, Di Fiore DP, Beltrame DF. The importance of evaluating patients with MINOCA (myocardial infarction with non-obstructed coronary arteries). Int J Cardiol. 2015;119:386–8.
2 Ghosh Dastidar A, Jonathan CL Rodrigues, Baritussio A, Bucciarelli-Ducci C. MRI in the assessment of ischaemic heart disesase. Heart. 2016;102(3):239–52.
3 Bulluck H, Maestrini V, Rosmini S, Abdel-Gadir A, Treibel TA, Castelletti S, et al. Myocardial T1 mapping. Circ J. 2015;79(3):487–94.
4 Ghosh Dastidar A, Rodrigues JC, Ahmed N, Baritussio A, Bucciarelli-Ducci C. The Role of cardiac MRI in patient with troponin-positive chest pain and unobstructed coronary arteries. Curr Cardiovasc Imaging Rep. 2015;8(8):28.