A 71-year-old woman presented with severe symptomatic sinus node dysfunction (with sinus pauses for up to 7 seconds and an average heart rate of 47 bpm on the Holter recording) with exertional dyspnoea and malaise. In 1974, she had a Dacron bypass implanted between the innominate vein and the right atrium for superior vena cava syndrome due to a mediastinal liposclerosis. The patient was on long-term warfarin therapy. She came to our hospital in March 2012 for a pacemaker implantation.
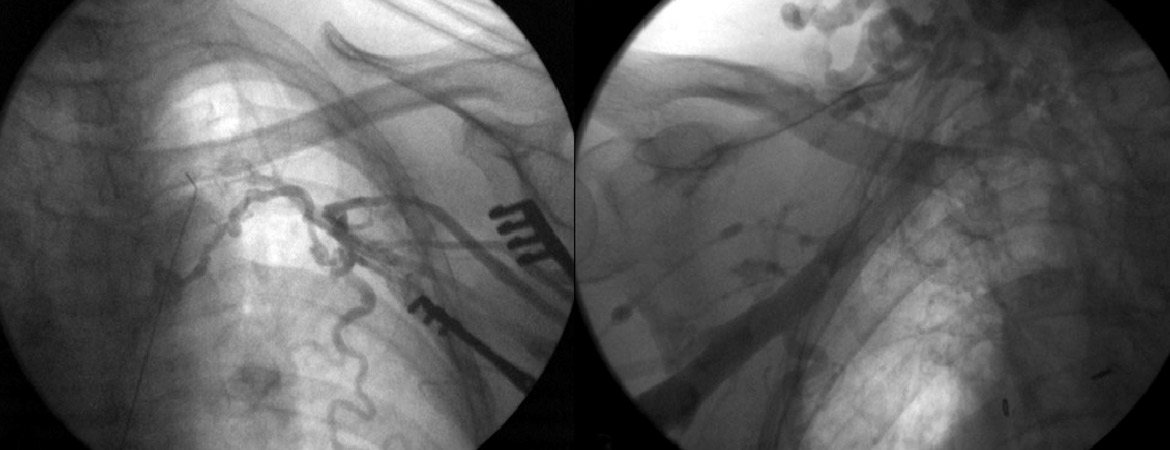
An initial approach via axillary and left subclavian venous puncture was attempted but was impossible owing to complete occlusion of this venous axis (fig. 1A). A venogram showed an occlusion of the right subclavian vein also (fig. 1B). Computed tomographic angiography indicated an obstruction of the superior vena cava and of the azygos arch with a collateral network draining through the azygos and hemiazygos network.
Figure 1: Obstruction of the left (A) and right (B) venous subclavian networks, visualised during intraoperative fluoroscopy.
The following options were then considered:
– Surgical access, either with epicardial leads or endocardial leads with a trans-atrial access. However, this was felt to be complicated due to fibrosis, secondary mediastinal liposclerosis and previous thoracic surgery.
– The second option, which was chosen, was to implant a transvenous atrial lead via femoral access.
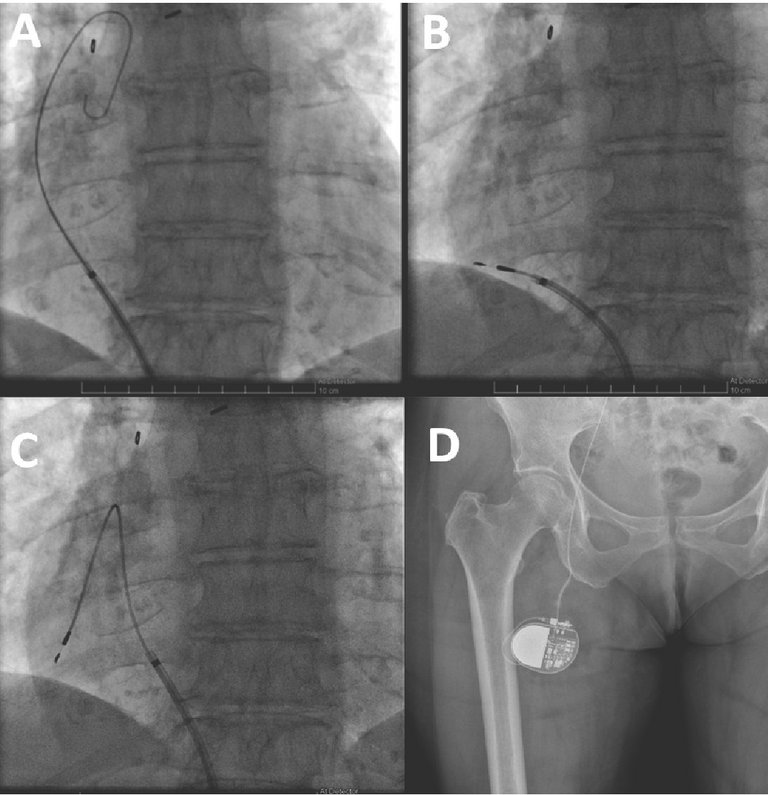
Pacemaker implantation: The right femoral vein was punctured in the groin, approximately 3 cm below the iliac ligament. A deflectable 8.4F guiding catheter (Medtronic® Minneapolis, MN, USA) was advanced over a 0.35 inch guidewire into the right atrium. A 69 cm Medtronic Select Secure 3830 lead was implanted in the right atrial appendage (figs 2 and 3). This is a 4.1 French lumenless fixed-helix active-fixation pacing lead that requires a guiding catheter for positioning. This model was chosen because of its length (59 cm and 69 cm available), its stability, and its high flexibility and tensile strength to accommodate increased stress due to hip flexion. The electrical parameters were normal and atrial pacing at 130 bpm revealed 1:1 conduction (with normal QRS width). For this reason, and to avoid excess foreign body material, a ventricular lead was not implanted. The lead was connected to a Medtronic Relia SR pacemaker, which was placed in a pocket in the upper anterior thigh. The wound was closed with resorbable subcuticular monofilament suture and a waterproof dressing was applied.
Figure 2: Device implantation. (A) Deflectable guiding catheter positioned in the right atrium over a guidewire via the right femoral vein. (B) Lead insertion into the right atrium via the guiding catheter. (C) Formation of a loop to allow sufficient slack and stabilise the lead. (D) Generator positioning in the superior and anterior part of the right thigh.
Figure 3: Chest X-ray of the pacing lead implanted in the right atrium via femoral venous access.
The patient was discharged on the day after the procedure, with the device programmed to AAIR 60–120 bpm. The wound healed well, without any discomfort caused by the generator pocket (fig. 4). The patient had marked symptomatic improvement, with rate histograms showing good adaptation despite the unusual generator location (fig. 5). Follow-up for more than 4 years has been uneventful, with stable electrical parameters.
Figure 4: The scar (highlighted by the dotted circle) on the right thigh, during follow-up a year after implantation and interrogation of the device by the programmer header.
Figure 5: Rate histogram showing the good adaptation of the device.
Discussion
The iliofemoral approach for pacemaker implantation has been described since the 1980s [1], but remains little known. The indications are most frequently a superior vena cava or subclavian / internal jugular axis obstruction. Rarely, congenital anomaly of venous return, infectious problems or wound healing at the pre-pectoral level may be the indication. Even biventricular pacemaker implantations have been described [2, 3].
Pacemaker implantation via the femoral vein is technically simple and accessible for every physician trained in cardiac stimulation. The Select Secure 3830 lead is particularly well suited for this purpose, for the reasons previously mentioned. However, a long (e.g., 65 cm) screw-in lead is also available from most manufacturers on demand.
A controversial point is the site of femoral puncture, which can be either above the inguinal ligament (avoiding potential lead crush, but exposing the patient to a risk of intestinal lesions and peritoneal bleedings) or below the ligament (which is easier and probably safer). Another point of debate concerns the generator pocket, which can be placed subcutaneously either in the inferior abdominal wall or in the superior part of the thigh, as for our patient, in order to avoid any supplementary stress on the lead during hip flexion.
The most frequently reported complication is atrial lead dislodgement, which is described in up to 20% of patients [4]. In order to reduce tension on the lead, it is suggested to form a loop in the atrium, as we did for our patient [5]. Another complication is lead fracture or insulation erosion, given the mechanical constraints on the lead in this area. The 3830 Select Secure lead, with its low profile and high tensile strength and flexibility, is well suited for this purpose. Finally, as for every device implantation, but especially in the groin area, meticulous attention must be paid to avoid infection.
This case also illustrated the utility of performing a venogram before a puncture is attempted (ideally even before skin incision if there is reason to suspect occlusion). To this purpose, we routinely equip our patients with an ipsilateral venous catheter before device implantation.
The advent of intracardiac pacemakers with femoral access (introduced in Switzerland in 2015) now offers a further option in case of venous access issues via the superior route. However, these are, for the time being, available only as single-chamber ventricular devices, and would have been suboptimal in our patient due to loss of atrioventricular synchrony. As generator changes are impossible for intracardiac pacemakers, femoral access for conventional pacemakers may be a preferable option for younger patients who will require many years of pacing therapy.
Conclusion
The femoral approach for pacemaker implantation is a simple solution that remains little known. It is a possibility to consider in cases with superior venous access issues and as an alternative to intracardiac pacemakers when atrial pacing is indicated.
Disclosure statement
No financial support and no other potential conflict of interest relevant to this article was reported.
Correspondence
Correspondence: MD Haran Burri Cardiology Department University Hospital of Geneva Rue Gabrielle Perret Gentil 4 CH-1211 Geneva 14 haran.burri[at]hcuge.ch
References
1 Ellestad MH, Caso R, Greenberg PS. Permanent pacemaker implantation using the femoral vein: a preliminary report. Pacing Clin Electrophysiol PACE. 1980;3(4):418–23.
2 Yousef Z, Paul V, Leyva F. Cardiac resynchronization via the femoral vein: a novel method in cases with contraindications to the pectoral approach. Europacce. 2006;8(2):144–6.
3 Agosti S, Brunelli C, Bertero G. Biventricular Pacemaker Implantation via the Femoral Vein. J Clin Med Res. 2012;4(4):289–91.
4 Mathur R, Stables RH, Heaven D, Ingram A, Sutton R. Permanent pacemaker implantation via the femoral vein: An alternative in cases with contraindications to the pectoral approach. Europace. 2001;3(1):56–9.
5 Tsutsumi K, Hashizume K, Kimura N, Taguchi S, Inoue Y, Kashima I, et al. Permanent pacemaker implantation via the iliac vein: an alternative in 4 cases with contraindications to the pectoral approach. J Arrhythmia. 2010;26(1):55–61.