Arrhythmias are the most common reason for hospital visits for grown-up congenital heart disease (GUCH) patients [1]. For these vulnerable patients, arrhythmias can be a sign of haemodynamic decompensation, or can themselves result in rapid decompensation. Arrhythmias that are relatively innocuous in other patients can be severely compromising in the GUCH population, whose cardiovascular haemodynamics are often precariously balanced.
As in the general population, the spectrum of ventricular arrhythmias in patients with congenital heart disease (CHD) ranges from ventricular ectopics to nonsustained ventricular tachycardia (VT), sustained monomorphic VT, polymorphic VT and ventricular fibrillation (VF). Accordingly, the clinical manifestations can be variable and include palpitations, syncope, heart failure secondary to tachycardiomyopathy, or sudden cardiac death (SCD) from malignant ventricular arrhythmias. The incidence of sudden cardiac death in the CHD population in general is estimated to be about 0.1% per year [2]. Sudden cardiac death (20%) and heart failure (30%) account for nearly half of all late deaths in mixed cohorts of children and adults with CHD [3]. Although nonsustained VT has not been linked to sudden death in a heterogeneous population of patients with CHD, it has been associated with inducible and clinical ventricular tachyarrhythmias in patients with tetralogy of Fallot (TOF) [4].
This article provides an overview of the electrophysiological treatments of ventricular arrhythmias in the setting of congenital heart disease.
Arrhythmogenic milieu in CHD patients
Underlying CHD often results in pathological ventricular hypertrophy, dilatation and/or fibrosis of either or both ventricles, and heart failure. As a result, in much the same way as with other diseases leading to ventricular remodelling and heart failure, the majority of sustained ventricular arrhythmias are polymorphic VT or ventricular fibrillation. Monomorphic sustained VT, however, is uncommon in the absence of a ventricular scar: for example, after atrial switch for d-transposition of the great arteries (d-TGA), sustained monomorphic VT occurred with an incidence of 0.5% per year, whereas polymorphic VT/VF were the most frequently recorded arrhythmias in these patients when implanted with an implantable cardioverter-defibrillator (ICD) [5].
In the preoperative state, the haemodynamic consequences of atrioventricular and great arterial valvular regurgitation or outflow obstruction result in ventricular dilatation, dysfunction, hypertrophy, ischaemia and fibrosis. The occurrence of coronary artery anomalies, atrioventricular nodal and conduction system abnormalities, the metabolic milieu (hypoxia, acidosis), and the haemodynamic-rheological burden of polycythaemia can all contribute to the proarrhythmic environment. After surgery, a patient may develop haemodynamic overload in other chambers or worsening of existing burdens, secondary valvular abnormalities, coronary injuries, injury to the atrioventricular node and conduction system or the haemodynamic and electrophysiological effects of the ventricular incision. Metabolic and electrolyte abnormalities, drug effects, systemic illnesses and inflammation can also play an important role at different times.
In patients with CHD, the burden of the original cardiac malformation is frequently combined with the sequellae of reparative surgery, and this combination increases these patients’ vulnerability to arrhythmias. After reparative surgery, the presence of surgical scars and prosthetic and patch material modifies mechanical and electrical properties of the ventricles by producing large inexcitable areas with adjoining, relatively delimited isthmuses of slowed conduction. This combination, as is well known at the atrial level, lends itself readily to monomorphic reentrant ventricular arrhythmias. Accordingly, in patients with repaired TOF and an ICD, more than 80% of all treated ventricular arrhythmias have been monomorphic VTs [5, 6]. Similarly, monomorphic VTs have also been reported in patients with d-TGA and ventricular septal defect (VSD) closure or repaired outflow tract obstruction. The presence of iatrogenic scars, however, does not exclude the occurrence of polymorphic VT/VF in these patients; since residual defects (VSD or outflow obstruction) or postsurgical sequelae (e.g., pulmonary regurgitation) still produce ventricular hypertrophy, fibrosis and dilatation and heart failure, which is thought to be the substrate for polymorphic VT/VF.
Because of the generally downhill course of the natural history of most severe congenital heart disease states, in particular uncorrected ones, there is a significant time-dependent increased risk of ventricular arrhythmia. Both the underlying disease and the type of surgical/interventional correction can significantly influence this risk. The lifetime estimated risk of ventricular tachycardia ranges from <2% for atrial septal defect to 10–15% for TOF with the caveat that these figures also reflect the average lifespan for patients with these conditions in addition to the disease itself [2]. In the absence of a surgical scar or patch, systemic ventricular dysfunction is the dominant underlying predictor for sudden cardiac death in CHD patients, typically due to polymorphic VT or VF. Compare, for instance, the 7–9% estimated lifetime incidence of VT in d-TGA after atrial switch (with a systemic right ventricle, prone to late failure) with an incidence of <2% for d-TGA after an arterial switch [2]. Recent data indicate that heart failure is on par with or gaining against sudden cardiac death as the chief cause of late death in a mixed CHD population [3], probably as a consequence of increasing life expectancy and perhaps also of improved management of malignant ventricular arrhythmias. As with other categories of heart disease, the decision to implant an ICD in patients with CHD should factor in overall life expectancy, and the risk of heart failure and comorbidities.
Therapies for ventricular arrhythmias
Therapy for ventricular arrhythmias in the setting of CHD includes specific reparative treatment of the underlying heart disease, and of the residual lesions, control of heart failure and treatment of comorbidities, as well as direct treatment of the ventricular arrhythmias. A case-by-case consultative interaction between electrophysiologists, heart failure specialists and GUCH specialists, as in our institution, can provide the close coordination and specific adjustments required for managing these complex patients.
Direct treatment modalities for ventricular arrhythmias include, of course, antiarrhythmic drugs, cardiac implantable devices including ICDs, and catheter and surgical ablation directed at the arrhythmia mechanism. Cardiac resynchronisation by itself is considered a heart failure management therapy and will not be detailed further here.
How can the electrophysiologist help?
Electrophysiologists can play an important and often a key role in diagnosing various arrhythmias and analysing their mechanisms. They can help in providing a prognostic risk stratification of arrhythmic death, and allow knowledgeable decision-making in the choice of appropriate therapy, in providing and implementing catheter ablation, and in counselling the patient on appropriate lifestyle choices, including leisure and professional pursuits as well as personal choices such as parenthood. Additionally, the electrophysiologist can provide specialised electrical therapy (cardiac resynchronisation) for the treatment of associated heart failure and can provide input to the cardiac surgeon in order to mitigate the arrythmogenicity of surgical scars or guide the surgeon to modify the scars in therapeutically useful ways, such as extending a scar to a nonexcitable boundary such as the pulmonary valve annulus during a surgical revision for right ventricular outflow obstruction.
In the acute situation, when faced with a VT in a patient with CHD, standard guideline-based management applies. Sustained ventricular arrhythmias should certainly be terminated expeditiously, particularly in patients with complex CHD and/or precarious haemodynamics. In most instances, electrical cardioversion or defibrillation is the preferred treatment option. In patients with CHD, it is useful to remember to modify external defibrillation paddle or pad positioning according to the position of the heart (e.g., dextrocardia). And in patients with intracardiac devices, the paddles/pads need to be placed at a distance of at least 8 cm away from the generator. Drug treatment for cardioversion of sustained VT may be considered in the rare patient with stable haemodynamics and a well-tolerated arrhythmia without significant ventricular scar or remodelling. Long-term drug treatment of ventricular arrhythmias is often limited by the extent and severity of ventricular remodelling, the risk of proarrhythmia and heart failure, and drug-specific long-term side effects. There is not much of an evidence base to fall back upon in this patient cohort and our experience has centred around amiodarone and sotalol as specific agents and beta-blockers as adjuvant treatment when possible. Clearly, safe and effective antiarrhythmic drug therapy is an unmet need, possibly even more pronounced in this cohort of patients. A more detailed discussion of antiarrhythmic drug therapy can be found elsewhere [4].
Arrhythmia evaluation
Holter monitoring for the detection of nonsustained and sustained ventricular arrhythmias should be considered in those adult CHD patients at high risk, including TOF (over 35 years of age), TGA-atrial switch or Fontan palliation. Implantable loop recorders may also be useful for evaluating recurrent but fleeting symptoms in these high risk patients.
The best studied subgroup of patients is those with repaired TOF in whom a number of features have been found to be associated with a high risk of malignant ventricular arrhythmias and/or SCD. They include older age at repair, transannular repair with or without right ventricular dysfunction-dilatation, significant pulmonary regurgitation, left ventricular dysfunction-dilatation, severe or increasing QRS prolongation, atrial arrhythmias, syncope, nonsustained VT, or inducible malignant sustained ventricular arrhythmias [6–8]. Patients with multiple risk factors even without arrhythmias can be considered for an electrophysiological (EP) study in order to improve risk stratification and even to evaluate possible interventional treatment.
In patients with implanted devices, additional diagnostic and therapeutic options have become available, including device monitoring for arrhythmia detection, diagnosis and burden estimation, noninvasive EP studies to evaluate inducibility and risk stratification, as well as overdrive pacing for terminating VT. After surgical repair, patients frequently demonstrate a wide QRS even in sinus rhythm, thus rendering the distinction of supraventricular from ventricular arrhythmias even more difficult, and electrogram information from implanted devices can be very helpful in this respect.
Electrophysiological studies
An EP study including programmed stimulation that demonstrates inducible sustained ventricular arrhythmias may indicate an arrhythmogenic ventricular substrate and, in some subsets of patients, a higher risk of malignant ventricular arrhythmias including clinical VT and sudden death [2]. The EP study also allows evaluation of sinus node function, atrioventricular nodal and infranodal conduction, as well as supraventricular arrhythmia inducibility. In most centres today, an EP study is usually performed with a view to a subsequent therapeutic option, whether catheter-based or intra-operative.
An EP study is indicated particularly in patients with unexplained syncope, resuscitated sudden death or potentially life-threatening arrhythmias and a high risk CHD substrate. If haemodynamically significant sustained ventricular arrhythmias can be induced, ICD implantation may be considered. An EP study should be considered particularly when a therapeutic option (catheter ablation) could be performed during the same procedure. The therapeutic-diagnostic yield of an EP study may also depend upon the underlying specific CHD substrate. There is limited data derived from subgroup analysis suggesting that inducible VT does not predict clinical outcomes in patients with TGA and intra-atrial baffles. [9]; nevertheless, even in these patients EP studies may have a role in assessing atrial arrhythmia inducibility and tolerability, and in evaluating the atrioventricular conduction system. Atrial arrhythmias in this subgroup could, in fact, trigger ventricular tachycardias and sudden death, possibly owing to rapid atrioventricular conduction concurrent with exertion resulting in haemodynamic instability from the atrial tachyarrhythmia itself or by secondary degeneration into a malignant ventricular tachyarrhythmia [2].
In CHD patients with significant ventricular arrhythmias, syncope or resuscitated sudden death and who are scheduled for surgery, an EP study should be considered in order to evaluate possible integration of therapy directed at the specific arrhythmia substrate during the surgical repair – intraoperative ablation or incisional lesions (see later). In some CHD patients, particularly those with a surgical ventricular scar, an EP study may also be required to reliably distinguish supraventricular arrhythmias.
Catheter ablation for ventricular tachycardia
The current state of the art of catheter ablation for VT has evolved considerably, but its efficacy is still limited by the inability to delineate the detailed electrical activation sequence and the complete reentrant circuit of the ventricular arrhythmia, either because it is intra-mural or more frequently, the “mapping” is precluded by haemodynamic compromise during sustained ventricular arrhythmia. Considerable progress has been made, however, in delineating potential “isthmuses” (“alley-ways” of pronounced slow conduction which play a key role in permitting the existence and stability of reentrant circuits) during sinus rhythm or a paced ventricular rhythm, particularly in patients with other forms of structural heart disease such as ischaemic and nonischaemic cardiomyopathies [10, 11]. These techniques can be applied to patients with operated CHD as well. The therapeutic aspect of catheter ablation relies upon the acute creation of electrically inactive myocardium (as a result of thermally mediated coagulative necrosis), but typically has a limited spatial extent (nontransmural and/or noncontiguous) and a nonnegligible component of reversible tissue injury. Therefore, ineffective ablation may be the result of inaccessible or unlocalisable isthmuses, noncontiguous/nontransmural coagulative necrosis, or tissue oedema instead of irreversible necrosis. Advances in catheter ablation technology, including irrigated radiofrequency ablation and, more recently, real-time contact force sensing [12] combined with 3D localisation, are thought to have resulted in significant improvements in ablation efficacy, although prospective long-term data are lacking.
Sustained monomorphic VT is most frequently related to a substrate composed of scar, anatomical obstacles and slow-conducting myocardium. This correlates well with the high incidence of sustained monomorphic VT in CHD patients with a surgical ventriculotomy, such as patients after corrective surgery for TOF. The majority of these VTs are fast and haemodynamically poorly tolerated (precluding detailed mapping during the arrhythmia) and therefore requiring a substrate- based ablation approach [7]. In repaired TOF patients, the surgical right free wall ventriculotomy, the ventricular septal defect (VSD) patch, the tricuspid valve and the pulmonary valve together result in multiple candidate isthmuses of which four are discrete and amenable to catheter ablation. In the typical case, an isthmus is formed between the right ventriculotomy or patch and the tricuspid annulus (no. 1). If the right ventriculotomy/patch does not traverse the pulmonary valve, the intervening tissue from the superior end of the scar to the pulmonary valve annulus forms another discrete isthmus (no. 2). A third lies between the superior border of the VSD patch and the pulmonary valve annulus (no. 3), whereas the fourth is formed between the VSD patch and the tricuspid annulus (no. 4) [13]. In post-mortem series of repaired TOF, isthmuses 3 and 1 were present in almost all specimens, whereas isthmuses 2 and 4 were observed in only 25 % and 13 %, respectively. In specimens from patients aged ≥5 years at the time of death, isthmus 3 was significantly narrower and thinner with more interstitial and replacement fibrosis than isthmus 1 [13, 14].
Macro-reentry using these isthmuses is the most frequent mechanism of sustained monomorphic VT in these patients and, depending upon the exit site (right ventricular free wall or septal) can produce different ECG morphologies (e.g., a characteristic QS or QR, respectively, in V1).
Anatomical and surgical variations can result in inter-individual differences in isthmus dimensions; for example, a transannular ventriculotomy abolishes the isthmus between the pulmonary valve and the superior limit of the ventriculotomy. Similarly, variations in VSD morphology and location can alter the dimensions of the surrounding isthmuses. Although slow conduction is well known to be a mandatory requirement for the establishment of sustained reentry, only recently have detailed electrophysiological mapping studies established objective and sensitive demarcations of arrhythmogenic isthmuses, chiefly by use of parameters of conduction velocity. Kapel et al. performed a detailed EP study including right ventricular endocardial voltage and activation mapping in these patients and were able to show that sustained monomorphic VT was either inducible, or occurred spontaneously and was inducible only when the involved isthmus(es) exhibited a conduction velocity below 0.5 m/sec. The isthmuses in these patients with inducible or both spontaneous and inducible sustained monomorphic VT were significantly narrower and longer and produced fractionated electrograms during sinus rhythm (or right ventricular pacing) [15]. These isthmuses could be successfully targeted by radiofrequency catheter ablation, resulting in termination of sustained VT and VT noninducibility with complete conduction block in sinus rhythm. Kapel et al. further showed the prognostic importance of targeting these isthmuses, since none of the patients lacking or with successful ablation of the slow conducting isthmuses developed recurrent or spontaneous sustained monomorphic VT during 262 patient-years of follow-up. Although based on a limited number of patients from three centres, these results are very promising and suggest the possibility of relatively simple individualised risk stratification in these patients based on right ventricular endocardial mapping. Furthermore, catheter ablation could also be utilised as primary prevention by ablating potentially arrhythmogenic isthmuses, although the utility and safety of this approach remains to be shown. On the other hand, identification of a select group of low-risk patients in whom catheter ablation may be performed without ICD implantation is likely to be challenging.
With the introduction of a combined transatrial-transpulmonary approach and only limited patch augmentation for pulmonary valve stenosis, anatomical isthmuses 1 and 2 may be prevented in the majority of patients. However, isthmus 3 will remain. Evaluation of its potential arrhythmogenicity with electroanatomic mapping is appealing, and could allow personalised risk stratification and tailored treatment for contemporary patients with repaired TOF. Whether preventive transection of isthmus 3 during initial repair is feasible and safe needs careful, multidisciplinary consideration.
Patients with a repaired TOF and high risk features or suggestive symptoms may benefit from this approach of stratification and primary prevention by catheter ablation. In addition, EP evaluation of potential isthmuses may also help guide surgical incision making and/or adjunctive cryotherapy if revision surgery is necessary. In some patients, therefore, an EP study may help to decide if surgical treatment of arrhythmias is necessary or can be useful. During the EP study, mapping of the arrhythmia substrate can help the surgeon “design” an effective incisional or intraoperative ablation lesion. Intraoperative cryoablation of the infundibular septum between the VSD patch and pulmonary annulus during surgical repair of TOF has been proposed, but neither efficacy nor safety (from proarrhythmia) have been evaluated.
Radiofrequency catheter ablation of VT in these patients remains challenging owing to the variable anatomy with occasionally difficult or limited access (occluded femoral vessels, interrupted inferior vena cava, surgically created obstacles, prostheses and baffles), the sometimes hypertrophied myocardium and a complex and highly variable arrhythmogenic substrate that is dependent on the original malformation and the type of repair that has been performed. Preexisting anatomical or surgical obstacles and associated or resultant fibrosis may render effective catheter ablation difficult, and alternative approaches, such as from the systemic arterial side of the circulation into the subaortic ventricle, may be effective [16].
Published results of ventricular tachycardia ablation in adults with CHD have obvious limitations, including small numbers as well as mixed substrate populations, thus restricting the value of estimates of arrhythmia-free survival [13].
Because the correlation between sustained monomorphic VT and sudden death remains imprecise, and because the risk of recurrence even after acutely successful ablation remains relatively high, VT ablation is only rarely seen as a substitute for ICD therapy, and most commonly as an adjunct to reduce multiple ICD shocks, for example for a VT storm.
Catheter ablation of VT in adults with CHD can also be considered as an alternative to drug therapy in patients with an ICD and symptomatic VT, and may also be reasonable for nonsustained VT or relatively well tolerated VT when targeting anatomical isthmuses (see below) or for frequent ectopy with progressively worsening ventricular function. Much more rarely, ablation can be helpful for resolving the haemodynamic risk in patients with slow but incessant tachycardias.
Sudden cardiac death and implantable cardioverter defibrillators in congenital heart disease
The incidence of SCD in repaired CHD is 0.9 per 1000 patient years, which is 25- to 100-fold higher than for the general population [5].
ICD interrogation in patients with repaired TOF and TGA, implanted for both primary and secondary prevention, has shown that >80% of all ventricular arrhythmias that prompted ICD therapy in repaired TOF and around 50% in TGA patients are fast and monomorphic VT, often with heart rates >200 bpm [8, 9].
Identifying risk factors in these patients is complicated by time- and age-dependent changes, such that factors identified in earlier series of patients may become less relevant to younger cohorts. Risk estimates also change as patients age and progress further along their disease course.
Factors most consistently associated with SCD in TGA with Mustard or Senning baffles include systemic ventricular dysfunction, severe tricuspid regurgitation, prolonged QRS duration, and atrial tachyarrhythmias [3, 18]. Interrogation of ICDs implanted for primary prevention in TGA has, however, reported rather low rates of subsequent ventricular arrhythmias. For example, in a multicentre cohort in which 35% of patients had a systemic right ventricular ejection fraction <35%, the appropriate ICD shock rate was 0.5% per year [9]. It may be that the 35% threshold value for primary prevention in case of a systemic left ventricle is not applicable to a systemic right ventricle, since normal values for a subpulmonary right ventricle are 20% lower than for a systemic left ventricle. To date, there are only limited data on patients with univentricular hearts who represent a minute fraction (<2%) of ICD recipients with CHD [19].
As with other pathologies, ICD implantation is indicated for secondary prevention of symptomatic, haemodynamically significant VT, and resuscitated sudden death due to malignant ventricular arrhythmias. It is also indicated for primary prevention in CHD with biventricular physiology, systemic left ventricular dysfunction (<35%) and New York Heart Association grade II or III symptoms. ICD implantation may be reasonable in TOF patients at high risk of sudden death even in the absence of spontaneous sustained malignant ventricular arrhythmias. In a multicentre study of 252 patients with TOF who underwent programmed ventricular stimulation, inducible sustained ventricular tachycardia was independently associated with a nearly 5-fold higher rate of clinical ventricular tachycardia or sudden cardiac death on follow-up [20]. However, as indicated earlier, in the absence of a ventricular scar, for example in patients with transposition and atrial baffles, inducible VT does not appear to predict clinical events and thus the value of programmed stimulation in these patients is unclear.
Young adults with CHD today are quite likely to outlive or find redundant or obsolete current-generation devices and leads, thereby necessitating complex and sometimes dangerous extraction and multiple replacement procedures. Transvenous leads risk creating venous occlusion or embolic vascular events with a right to left intracardiac shunt, whereas epicardial and/or subcutaneous coils require a more invasive approach and have higher lead failure rates, as well as the possibility of a restrictive “pericardial” physiology related to defibrillation patches. The recently commercialised subcutaneous ICD system appears to be a favourable solution for patients in whom transvenous access is not feasible or desirable and in whom bradycardia and antitachycardia pacing features are not essential (since pacing is not possible). It may be compatible with a permanent pacemaker if pacing leads are bipolar and preimplant screening reveals the absence of T-wave oversensing during intrinsic and paced rhythms (frequent with the subcutaneous ICD) or eventually a leadless one. Regardless of the type of system implanted, however, inappropriate shocks are common in this population, occurring in 25% over 3 to 4 years of follow-up [19, 21].
Current implantable devices offer sophisticated programming options, and individualised programming can significantly reduce inappropriate and avoidable shocks. Inappropriate shocks are most commonly due to sinus tachycardia, supraventricular arrhythmias, T-wave oversensing, or lead failure, and can be reduced by adjuvant atrioventricular nodal blocking therapy or catheter ablation of supraventricular tachycardias (SVTs) (mostly intra-atrial reentrant tachycardias, often relatively slow with resulting frequent 1:1 atrioventricular conduction) [2].
Useful programming options to reduce avoidable shocks include antitachycardia pacing (ATP) and adjustment of detection time/intervals. ATP can be highly effective in terminating ventricular tachycardia without shocks in patients with CHD, and is therefore painless. It is safe, but sometimes causes VT acceleration, which is usually handled well by device safety algorithms and appropriate shocks if necessary. Longer detection delays for VF detection have also been found to be safe and effective in reducing the incidence of shocks. ATP can be programmed for slow and fast VT zones, as well as before or during charging.
Illustrative case
The following history may provide a useful example of many of the issues discussed above in the management of VT in the setting of complex CHD.
A 14-year-old boy with recurrent monomorphic VT was referred to our EP unit. He was born with a double-outlet right ventricle, d-TGA and a nonrestrictive VSD. He underwent an atrial septostomy and pulmonary artery banding in infancy, followed at 3 years of age by a Rastelli-type correction involving subaortic conal resection, patch closure of the VSD with creation of an internal hemi-tube establishing left ventricular outflow continuous with the aorta, and an external right ventricle to pulmonary artery conduit (mandated by an anomalous left anterior descending artery originating from the right coronary artery and crossing the anterior right ventricle). This conduit required percutaneous dilatation once and was surgically revised another time thereafter. Since the age of 7, monomorphic sustained VT recurred multiple times (fig. 1, left panel), despite antiarrhythmic drug treatment including sotalol and amiodarone, and required electrical cardioversions.
Figure 1: Left panel shows the clinical VT with a left bundle-branch block, left axis pattern and precordial transition in V5 compatible with a right ventricle free wall exit. Centre panel shows fluroscopic stills, anteroposterior (AP) view on top and left lateral below, with one catheter in the right pulmonary artery (PA) via the inferior vena cava, right atrium and right ventricle (RV) and a graduated pigtail catheter in the dextro-posed aorta and aortic root. White arrows indicate the calcified RV to PA conduit and the dashed white line indicates its junction with the RV. Right panel shows an electro-anatomical activation map of the RV, AP view on top and left lateral on the right. Orange hue indicates early activation and purple the latest activation, showing activation originating from the septal RV with later activation of the RV free wall and finally of the region close to the superior tricuspid annulus. Red dots indicate ablation lesions, delivered in a “linear” contiguous arrangement from the base of the conduit (grey zone indicating scar and the three blue dots) as well additionally at regions with fractionated and late potentials.
In our laboratory, an electroanatomic voltage map (fig. 2, right panel) and an activation map (fig. 1, right panel) of the right ventricle was created in sinus rhythm, confirming a low voltage zone with delayed activation in the septal outflow region, consistent with the VSD-left ventricular outflow patch, and another similar zone in the anterior outflow, consistent with the origin of the conduit to the pulmonary artery (fig. 1, middle panel: conduit indicated by white arrows on fluoroscopic views).
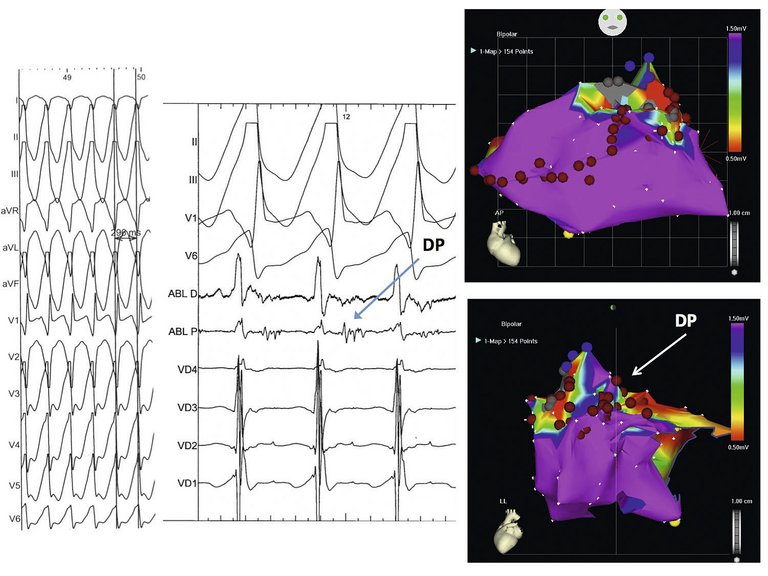
Figure 2: Left panel shows the ECG of the second VT (VT2), induced after creating the right ventricular (RV) free wall linear lesion, with a morphology indicating a septal superior exit (QR in V1, transition V3). Middle panel shows a recording during this VT at the septal junction of the RV summit with the conduit (white arrow in right panel). Recording shows, from top, leads II, III, V1 and V6 and from the ablation catheter placed at the septal RV summit showing prominent diastolic fractionated potentials (DP), larger in amplitude and sharper in the proximal electrodes of the ablation catheter (Abl p). Also shown are RV electrograms (VD1–4) with a clearly systolic timing. Right panel shows an electro-anatomic sinus rhythm voltage map with purple indicating bipolar endocardial voltage greater than 1.5 mV and all other colours a lower voltage, clearly centered around the base of the conduit and in the septal superior and peritricuspid region including the area where DPs were recorded during VT2.
The clinical VT demonstrated a left bundle-branch block and leftward axis configuration with a precordial transition indicating a right ventricular free wall exit. A sequence of contiguous radiofrequency lesions was created on the anterior wall of the right ventricle extending from the inferior border of the anterior zone, and continuing to the anterior border of the tricuspid annulus (fig. 1, left and right panels). Additional lesions were made in the narrow zone of normal-voltage tissue interposed between the septal and anterior scar zones. Inducibility testing confirmed that the clinical VT could not be induced, but a different sustained monomorphic VT was induced (VT2), with an inferior axis, QR morphology in V1 and a transition in V3, suggesting a septal superior exit, probably nearer the septal left ventricular outflow tract patch (figs 1 and 2, right panels) . Diastolic potentials were recorded on the right ventricular side of this region during on-going VT (fig. 2, centre panel), and because of proximity to the His bundle potential, radiofrequency lesions were prudently delivered to this region in sinus rhythm (fig. 3).
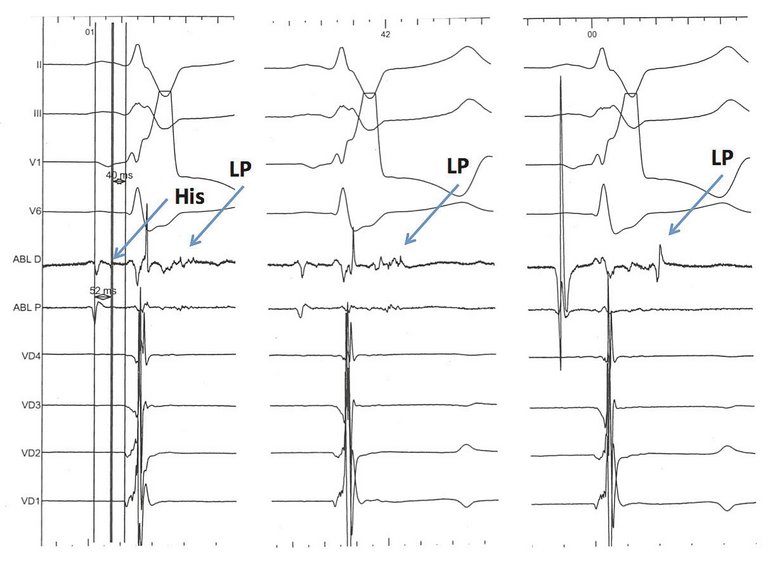
Figure 3: Abnormal late potentials in sinus rhythm. Three examples of fractionated, late potentials (beyond the terminal surface ECG QRS, LP) . Note the His bundle deflection in the tracing on the left side. These are electrograms indicating a candidate arrhythmogenic isthmus (see text).
Although a VT similar in morphology to the second VT remained inducible thereafter, no further attempts at ablation in this region or on its corresponding left side were made in view of the proximity to the atrioventricular conduction system and noninducibility of the clinical VT. A couple of weeks later, the conduit was surgically revised for haemodynamically significant stenosis and a single chamber ICD implanted without complications or arrhythmia recurrence. Over 5 years of follow-up, although he had an ICD intervention during early follow-up (unclear whether appropriate), he has been doing well for the last 3 years without antiarrhythmic therapy and without any further ICD intervention.
This patient illustrates many of the key issues relevant to ventricular arrhythmias in patients with complex CHD. The anatomical obstacles in this patient included the surgical scars of the implanted conduit, as well as the VSD-left ventricular outflow patch, with an intervening zone of low voltage tissue. The clinical VT compatible with a right ventricular free wall exit was probably related to a macro-reentrant circuit around the tricuspid annulus or around the conduit implantation site. The right free wall lesion, as shown in the images, was created to interrupt passage of electrical activation sustaining either or both of the above reentry circuits and accordingly could not be re-induced. However, the second VT manifested mid-diastolic potentials at the septal VSD-left ventricular outflow patch region, with a surface ECG indicating a septal exit, but could not be eliminated despite ablation at this site. It is likely that the critical pathway maintaining this VT was deep within the fibrous tissue at the edge of the septal patch, close to the His bundle and not susceptible to prudent radiofrequency-induced tissue heating from the right side. The inducibility of the residual VT, despite being non-clinical, prompted ICD implantation. Follow-up revealed no ICD intervention or VT during the last 3 years without antiarrhythmic drug treatment.
Clinical implications
As in other patients, ventricular arrhythmias are a major cause of morbidity and mortality in patients with CHD. Appropriate diagnosis and specific treatment can provide effective management for most patients with VT. Current expertise in diagnostic electrophysiology can lead to individualised recognition of current and potential arrhythmogenic tissue isthmuses, allowing in most cases their neutralisation by catheter ablation with resulting improvements in arrhythmia control and symptoms, although prognostic benefits have not yet been demonstrated.
Disclosure statement
No financial support and no other potential conflict of interest relevant to this article was reported.
Correspondence
Correspondence: Dipen Shah MD, FHRS Cardiac EP unit, Cardiology Service University Hospitals Geneva Rue Gabriel Perret Gentil 4 CH-1211 Geneve Dipen.shah[at]hcuge.ch
References
1 Kaemmerer H, Bauer U, Pensl U, Oechslin E, Gravenhorst V, Franke A, Het al. Management of emergencies in adults with congenital cardiac disease. Am J Cardiol. 2008;101:521–5.
2 Khairy P, Van Hare GF, Balaji S, Berul CI, Cecchin F, Cohen MI, et al. PACES/HRS Expert Consensus Statement on the Recognition and Management of Arrhythmias in Adult Congenital Heart Disease: developed in partnership between the Pediatric and Congenital Electrophysiology Society (PACES) and the Heart Rhythm Society (HRS). Endorsed by the governing bodies of PACES, HRS, the American College of Cardiology (ACC), the American Heart Association (AHA), the European Heart Rhythm Association (EHRA), the Canadian Heart Rhythm Society (CHRS), and the International Society for Adult Congenital Heart Disease (ISACHD). Heart Rhythm. 2014;11(10):e102–65.
3 Engelings CC, Helm PC, Abdul-Khaliq H, Asfour B, Bauer UM, Baumgartner H, et al. Cause of death in adults with congenital heart disease – An analysis of the German National Register for Congenital Heart Defects. Int J Cardiol. 2016;211:31–6.
4 Khairy P. Ventricular arrhythmias and sudden cardiac death in adults with congenital heart disease. Heart. 2016;102:1703–9.
5 Silka MJ, Hardy BG, Menashe VD, Morris CD. A population-based prospective evaluation of risk of sudden cardiac death after operation for common congenital heart defects. J Am Coll Cardiol. 1998;32:245–51.
6 Gatzoulis MA, Till JA, Somerville J, Redington AN. Mechanoelectrical interaction in tetralogy of Fallot. QRS prolongation relates to right ventricular size and predicts malignant ventricular arrhythmias and sudden death. Circulation. 1995;92(2):231–7.
7 Zeppenfeld K. Ventricular tachycardia in repaired congenital heart disease. Herzschrittmacherther Elektrophysiol. 2016;27(2):131–6.
8 Khairy P, Harris L, Landzberg MJ, Viswanathan S, Barlow A, Gatzoulis MA, et al. Implantable cardioverter-defibrillators in tetralogy of Fallot. Circulation 2008;117:363–70.
9 Khairy P, Harris L, Landzberg MJ, Fernandes SM, Barlow A, Mercier LA, et al. Sudden death and defibrillators in transposition of the great arteries with intra-atrial baflles: a multicenter study. Circ Arrhythm Electrophysiol. 2008;1:250–7.
10 Arenal A, Glez-Torrecilla E, Ortiz M, Villacastín J, Fdez-Portales J, Sousa E, et al. Ablation of electrograms with an isolated, delayed component as treatment of unmappable monomorphic ventricular tachycardias in patients with structural heart disease. J Am Coll Cardiol. 2003;41(1):81–92.
11 Jaïs P, Maury P, Khairy P, Sacher F, Nault I, Komatsu Y, et al. Elimination of local abnormal ventricular activities: a new end point for substrate modification in patients with scar-related ventricular tachycardia. Circulation. 2012;125(18):2184–96.
12 Shah DC, Namdar M. Real-Time Contact Force Measurement: A Key Parameter for Controlling Lesion Creation With Radiofrequency Energy. Circ Arrhythm Electrophysiol. 2015;(3):713–21.
13 Brouwer C, Hazekamp MG, Zeppenfeld K. Anatomical Substrates and Ablation of Reentrant Atrial and Ventricular Tachycardias in Repaired Congenital Heart Disease. Arrhythm Electrophysiol Rev. 2016;5(2):150–60.
14 Moore JP, Seki A, Shannon KM, Mandapati R, Tung R, Fishbein MC. Characterization of anatomic ventricular tachycardia isthmus pathology after surgical repair of tetralogy of Fallot. Circ Arrhythm Electrophysiol. 2013;6(5):905–11.
15 Kapel GF, Sacher F, Dekkers OM, Watanabe M, Blom NA, Thambo JB, et al. Arrhythmogenic anatomical isthmuses identified by electroanatomical mapping are the substrate for ventricular tachycardia in repaired tetralogy of Fallot. Eur Heart J. 2016, 26. pii: ehw202.
16 Kapel GF, Reichlin T, Wijnmaalen AP, Tedrow UB, Piers SR, Schalij MJ, et al. Left-sided ablation of ventricular tachycardia in adults with repaired tetralogy of Fallot: a case series. Circ Arrhythm Electrophysiol. 2014;7(5):889–97.
17 Verheugt CL, Uiterwaal CS, van der Velde ET, Meijboom FJ, Pieper PG, van Dijk AP, et al. Mortality in adult congenital heart disease. Eur Heart J. 2010;31:1220–9.
18 Kammeraad JA, van Deurzen CH, Sreeram N, et al. Predictors of sudden cardiac death after Mustard or Senning repair for transposition of the great arteries. J Am Coll Cardiol. 2004;44:1095–102.
19 Vehmeijer JT, Brouwer TF, Limpens J, Knops RE, Bouma BJ, Mulder BJ, de Groot JR. Implantable cardioverter-defibrillators in adults with congenital heart disease: a systematic review and meta-analysis. Eur Heart J 2016;37:1439–48.
20 Khairy P, Landzberg MJ, Gatzoulis MA, Lucron H, Lambert J, Marcon F, et al. Value of programmed ventricular stimulation after tetralogy of Fallot repair: a multicenter study. Circulation 2004;109:1994–2000.
21 Moore JP, Mondésert B, Lloyd MS, Cook SC, Zaidi AN, Pass RH, et al. Alliance for Adult Research in Congenital Cardiology (AARCC). Clinical Experience With the Subcutaneous Implantable Cardioverter-Defibrillator in Adults With Congenital Heart Disease. Circ Arrhythm Electrophysiol. 2016;9(9). pii: e004338. doi: 10.1161/CIRCEP.116.004338.