In July 2013, a 75-year-old man with known bilateral arthrosis presented at a local hospital with swelling and warmth of the left knee, fever over 39 °C and increased inflammation indicators. For further investigation, the left knee was punctured. Two lavages and synovectomies were performed. A first transthoracic echocardiography (TTE) confirmed good function of all valves without any hint of vegetations. Empirical antibiotic therapy was started with co-amoxicillin and gentamicin (table 1). The patient was discharged on co-amoxicillin after almost 3 weeks of hospitalisation. Streptococcus pneumoniae was detected in puncture samples. After 1 week, the patient was again admitted to a local hospital with persistent fever over 38 °C under antibiotic therapy, new cardiac decompensation with concomitant pleural effusion, and worsening of his general condition. The antibiotic therapy was changed to ceftriaxone. Swelling of the left knee was no longer significant. Transoesophageal echocardiography (TOE) revealed a mild insufficiency jet at the aortic valve, located in the area of the left cusp, that raised suspicion of a perforation. After diuretic therapy, the cardiac decompensation and his general condition were improved. In the meantime, the patient underwent regular echocardiographic follow-up, which showed clear progression of the moderate aortic valve insufficiency to a severe level, leading to transfer to the surgical department. The aortic valve operation was performed 3 days later, after 3 weeks of antibiotic treatment with co-amoxicillin and another week of ceftriaxone. Intraoperative findings were an infected aortic valve with mucous surface and perforation of the left coronary cusp. Because there was no abscess, the cusps of the aortic valve were excised and a 23-mm biological aortic valve prosthesis (St. Jude Medical, Trifecta) was implanted. The further course was uneventful and the patient was discharged to cardiac rehabilitation on the sixth postoperative day and received further antibiotic therapy with ceftriaxone for a cumulative period of 6 weeks after the operation.
Table 1: Antibiotic treatment during both infections.
Clinical/laboratory findings
Antibiotics
Dose
Sensitivity
Treatment period
First infection
Swelling of the knee Empyema, knee lavage
Co-amoxicillin
2.2 g i.v. 3× day
17.7.13–11.8.13
(per os)
(26.7.13–4.8.13)
Gentamicin
300 mg i.v. 1× day
19.7.13–22.7.13
S. pneumoniae (puncture samples) Endocarditis (perforation)
Ceftriaxone
2 g i.v. 1× day
Unknown
12.8.13–21.8.13
Penicillin G
4 Mio E 6 × day
22.8.13–27.8.13
Ceftriaxone
2 g i.v. 1× day
28.8.13–27.9.13
Second infection
Swelling of the knee Knee lavage and operation
Tobramycin
240 mg i.v 1× day
29.12.14
Vancomycin
1 g i.v. 2× day
29.12.14–5.1.15
Ciprofloxacin
400 mg i.v. 2× day
30.12.14–5.1.15
S. pneumoniae (blood cultures, samples)
Ceftriaxone
2 g i.v. 2× day
5.1.15–12.1.15
1× day
12.1.15–19.1.15
Endocarditis (vegetation)
Gentamicin
300 mg i.v. × day
13.1.15–19.1.15
Rifampicin
300 mg i.v. 3× day
13.1.15–19.1.15
Information regarding minimum inhibitory concentration
Penicillin G
6 × 4 Mio U
0.03 mg/l
19.1.15–2.3.15
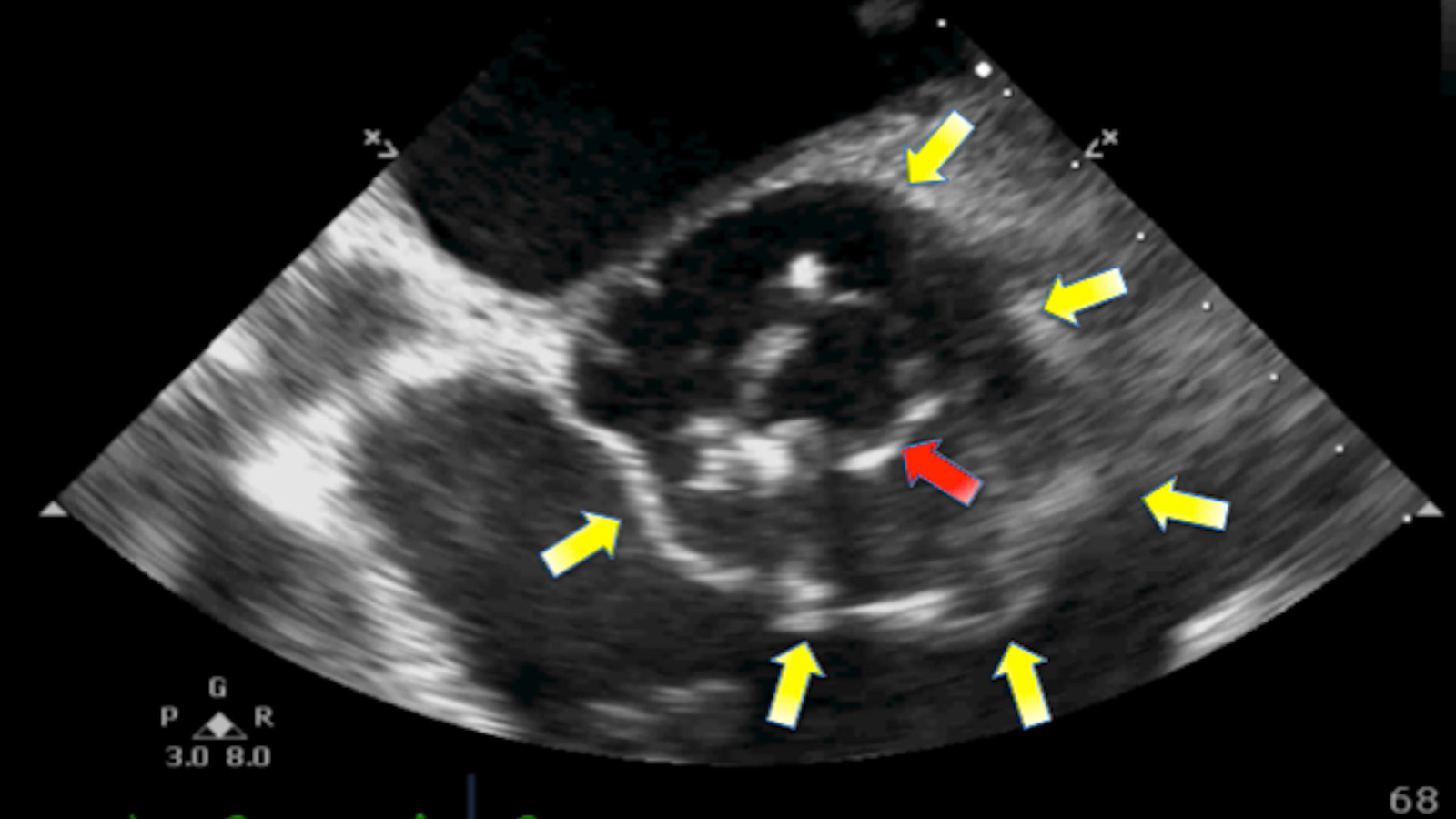
One year later, in June 2014, the patient received an endoprosthesis of the left knee because of the severe arthrosis. Cefazolin was administered as intraoperative prophylaxis. Initially, the postoperative course was uneventful; specifically, there was no need of antibiotic treatment. In December 2014, the patient presented again with a swelling of the left knee and fever. As a patient at high risk for endocarditis after valve replacement and endoprosthesis implantation, a TTE was performed immediately on admission and a TOE 2 days later, without signs of an abscess, vegetation or perforation and with a competent aortic valve prosthesis. Empirical therapy was started with vancomycin and ciprofloxacin on the admission day. Three days after the negative TEE, the patient was scheduled for lavage of the knee prosthesis and a change of the inlay for eradication of the local infection. Twelve days later a second TOE was indicated because of persistent inflammation under antibiotic therapy. Clinically, there was no sign of cardiac decompensation or any cardiopulmonary symptoms. The echocardiographic findings were a vegetation of 0.8 cm on the aortic valve prosthesis and a new periannular abscess (fig. 1). The ECG did not show any abnormalities due to the annular abscess and, especially, no signs of atrioventricular block. The analysis of the blood cultures and knee aspirate confirmed S. pneumoniae. Antibiotic therapy was changed to ceftriaxone complemented by rifampicin and gentamicin after diagnosis of the valve vegetation. Because of suspected endocarditis, transfer to the cardiac surgery department was organised.
Figure 1: TOE on second admission to cardiac surgery during relapse after implantation of knee prosthesis: annular abscess (yellow arrow) around the prosthetic valve (red arrow).
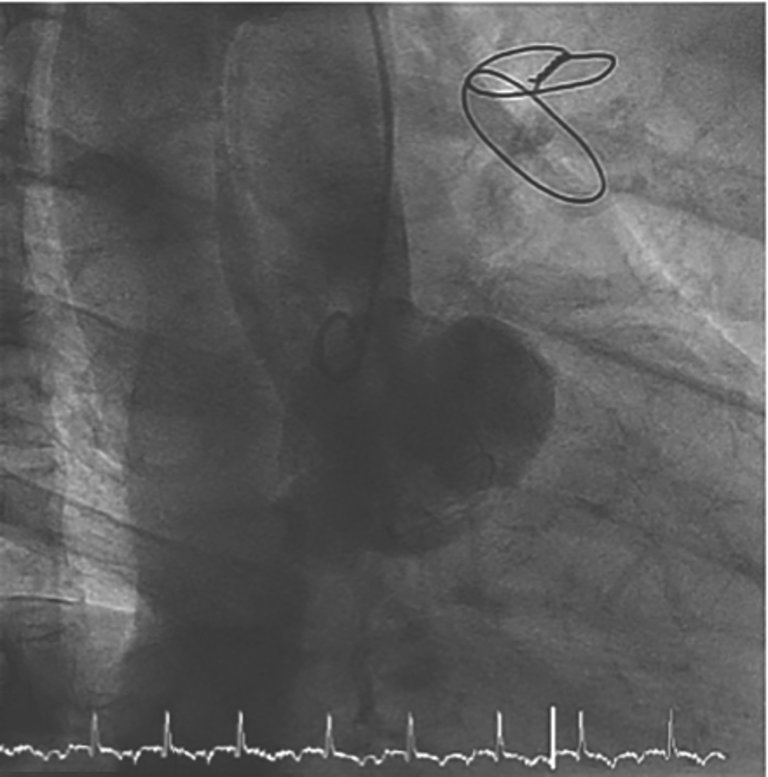
In this case the involvement of an endocarditis team was necessary to coordinate the following therapy. One week after adjustment of the antibiotics to penicillin, according to sensitivity analysis of the bacterium, the knee endoprosthesis was explanted in total. During the operation we performed a TOE, which showed an increase in the vegetation length to 1.6 cm. The following day preoperative diagnostic tests including computed tomography for exclusion of septic embolism and coronary angiography were performed (fig. 2). The patient was scheduled for cardiac operation 3 days after explantation of the knee prosthesis. Surprisingly, concerning cardiac complaints, the patient remained oligosymptomatic.
Figure 2: Coronary angiography: Contrast medium shows an enlargement of the aortic root without insufficiency.
Operation and findings
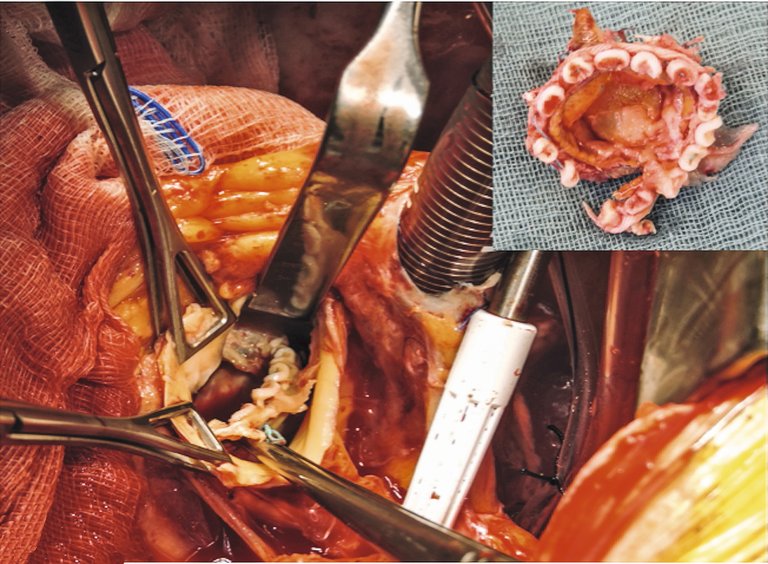
Intraoperative echocardiography showed a disconnection of the aortic valve prosthesis with a huge abscess surrounding the annular area (fig. 3a,b). For the first time, aortic insufficiency was diagnosed (fig. 3b). The biological aortic prosthesis could be removed without any difficulty only by elevation with forceps from the right coronary sinus, where the insufficiency was detected before. A large annular abscess had to be eradicated (fig. 4). Afterwards, a biological freestyle aortic root prosthesis (Freestyle, Medtronic) was implanted to avoid as much artificial material as possible. Additionally, epicardial pacemaker wires for the right atrium and right ventricle were implanted during the operation because of the high risk of atrioventricular block after eradication of the huge abscess.
Figure 4: Intraoperative view: The aortic prosthesis could be removed without any difficulty only by elevation with the forceps from the right coronary sinus, where the insufficiency was detected before.
Postoperative course
The patient was extubated after the operation on the same day. One day later he underwent cardiac pacing because of complete atrioventricular block. He recovered well and was mobilised despite the knee prosthesis explantation. Pneumococcus vaccine was given before discharge. After a total of 2 months the patient was admitted to cardiovascular and musculoskeletal rehabilitation, where he followed the training without the knee prosthesis and could climb about 50 steps with forearm crutches. In April 2016, almost 15 months after the explantation, the patient received a new prosthesis of his left knee without any difficulties. Cardiac follow-up care confirmed a normally functioning aortic prosthesis with a left ventricular function of 50%.
Discussion
This case report highlights the occurrence of two uncommon diseases that influenced each other and finally involved an interdisciplinary therapeutic approach. Currently, S. pneumoniae is an infrequent cause of severe infective endocarditis. In the pre-antibiotic era it was responsible for 15% of all cases of infective endocarditis, whereas in the 1980s and 1990s, prevalence was <3% [1]. Former case series have suggested that rare pneumococcal endocarditis is mostly reported in patients with co-morbidities but no underlying valve disease, and leads to rapid heart failure and a high mortality [2]. Several characteristics of pneumococcal endocarditis have been identified, and half of the cases developed concomitant pneumonia or meningitis [1]. The manifestation of endocarditis in our patient began with the knee infection. Although most cases of septic arthritis are caused by Staphylococcus aureus and Staphylococcus epidermidis, S. pneumoniae has been noted to cause up to 10% of reported cases and, currently, is being increasingly recognised [3, 4]. This trend demonstrates that in our future clinical practice we have to consider S. pneumoniae as a more common agent of septic arthritis and, consequently, its complications in elderly patients. Because S. pneumoniae infection is a droplet-transmitted disease, we hypothesise that the patient was exposed to droplet infection prior to the knee infection. Normally, this exposure leads to pneumonia or sinusitis. The development of an infective arthritis is a rarer, but familiar, course in elderly patients. An infection caused by dental procedures would be conceivable for Streptococcus mitis/oralis, but does not support our theory of the potential source.
The patient left hospital in August 2013 and received the knee prosthesis in June 2014. A relapse with the same bacterium 1 year after initial infection would be rare, but is still conceivable. The relapse might be supported by a suppressed immune status of the patient and, as in our case, a prosthetic joint [4]. During the first episode of endocarditis the knee infection no longer played a leading role because of good regression of the symptoms. That is why we did not focus on any invasive treatment of the knee during the first hospitalisation and after discharge. This condition of a non-eradicated, asymptomatic source of infection might support the theory of a later relapse. Nevertheless, reinfection with S. pneumoniae may be considered as well. A susceptibility to pneumococcal infection could explain a new reinfection during knee prosthesis implantation.
Typing of the bacteria might give the answer as to whether this was relapse or reinfection. Unfortunately, we did not arrange for specific typing of the pathogen during either the first or second infection. On the first admission of the patient to cardiac surgery, typing was not routine because of the lack of treatment consequences. On the second admission, blood samples had already been taken and analysed in the local hospital. Again, serotyping was not done.
The advantages of a freestyle prosthesis for root replacement in endocarditis have been discussed and are well-known, with good late survival, low rates of recurrence of endocarditis, immediate local control and good haemodynamic performance [5]. In younger patients, use of a homograft might be worth discussing.
One might say that earlier valve surgery was mandatory because of the large aortic root abscess [1]. Current guidelines define abscess formation as an indication for urgent operative treatment (IB). On the other hand, elimination of potential sources of sepsis at least 2 weeks before implantation of a prosthetic valve is recommended (IIa, C) [6]. Because of the patient’s stable condition, without aortic insufficiency, we considered the removal of the knee prosthesis an obligatory step before reoperation on the aortic root, 3 days later. We agree that in the case of cardiac decompensation and aortic insufficiency, or development of further symptoms, this wait-and-see tactic would not be feasible.
Conclusion
Infective endocarditis caused by Streptococcus pneumoniae remains a rare disease, which is becoming more relevant in the context of ageing population. Not only community-acquired pneumonia and meningitis, but also pneumococcal arthritis might be a more frequent infective focus in elderly patients in upcoming decades. Although it is classified as an uncomplicated bacterium, individual treatment to eradicate the infective focus and valve surgery have to be considered. In cases of abscess formation especially, short-term follow-up investigations are indicated, as pneumococcal endocarditis may rapidly progress, with high mortality.
Disclosure statement
No financial support and no other potential conflict of interest relevant to this article was reported.
1 de Egea V, Muñoz P, Valerio M, de Alarcón A, Lepe JA, Miró JM, et al. GAMES Study Group. Characteristics and Outcome of Streptococcus pneumoniae Endocarditis in the XXI Century: A Systematic Review of 111 Cases (2000-2013). Medicine (Baltimore). 2015;94(39):e1562. doi:.
2 Daudin M, Tattevin P, Lelong B, Flecher E, Lavoué S, Piau C, et al. Characteristics and prognosis of pneumococcal endocarditis: a case-control study. Clin Microbiol Infect. 2016;22(6):572.e5–8. doi:.
3 Belkhir L, Rodriguez-Villalobos H, Vandercam B, Marot JC, Cornu O, Lambert M, et al. Pneumococcal septic arthritis in adults: clinical analysis and review. Acta Clin Belg. 2014;69(1):40–6. doi:.
4 Roberts AL, Hewlett AL, Yu J, Nahm MH, Fey PD, Iwen PC. Streptococcus pneumoniae serotype 6C presenting as recurrent prosthetic knee joint infection in a patient with a history of congenital asplenia and underlying autoimmune disease: a case report and literature review. Diagn Microbiol Infect Dis. 2013;77(4):376–9. doi:.
5 Schneider AW, Hazekamp MG, Versteegh MI, Bruggemans EF, Holman ER, Klautz RJ, et al. Stentless bioprostheses: a versatile and durable solution in extensive aortic valve endocarditis. Eur J Cardiothorac Surg. 2016;49(6):1699–704. doi:.
6 Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. Document Reviewers. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075–128. doi:.
1 de Egea V, Muñoz P, Valerio M, de Alarcón A, Lepe JA, Miró JM, et al. GAMES Study Group. Characteristics and Outcome of Streptococcus pneumoniae Endocarditis in the XXI Century: A Systematic Review of 111 Cases (2000-2013). Medicine (Baltimore). 2015;94(39):e1562. doi:.
2 Daudin M, Tattevin P, Lelong B, Flecher E, Lavoué S, Piau C, et al. Characteristics and prognosis of pneumococcal endocarditis: a case-control study. Clin Microbiol Infect. 2016;22(6):572.e5–8. doi:.
3 Belkhir L, Rodriguez-Villalobos H, Vandercam B, Marot JC, Cornu O, Lambert M, et al. Pneumococcal septic arthritis in adults: clinical analysis and review. Acta Clin Belg. 2014;69(1):40–6. doi:.
4 Roberts AL, Hewlett AL, Yu J, Nahm MH, Fey PD, Iwen PC. Streptococcus pneumoniae serotype 6C presenting as recurrent prosthetic knee joint infection in a patient with a history of congenital asplenia and underlying autoimmune disease: a case report and literature review. Diagn Microbiol Infect Dis. 2013;77(4):376–9. doi:.
5 Schneider AW, Hazekamp MG, Versteegh MI, Bruggemans EF, Holman ER, Klautz RJ, et al. Stentless bioprostheses: a versatile and durable solution in extensive aortic valve endocarditis. Eur J Cardiothorac Surg. 2016;49(6):1699–704. doi:.
6 Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. Document Reviewers. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075–128. doi:.